by Michael Passwater
Orthomolecular Medicine News Service
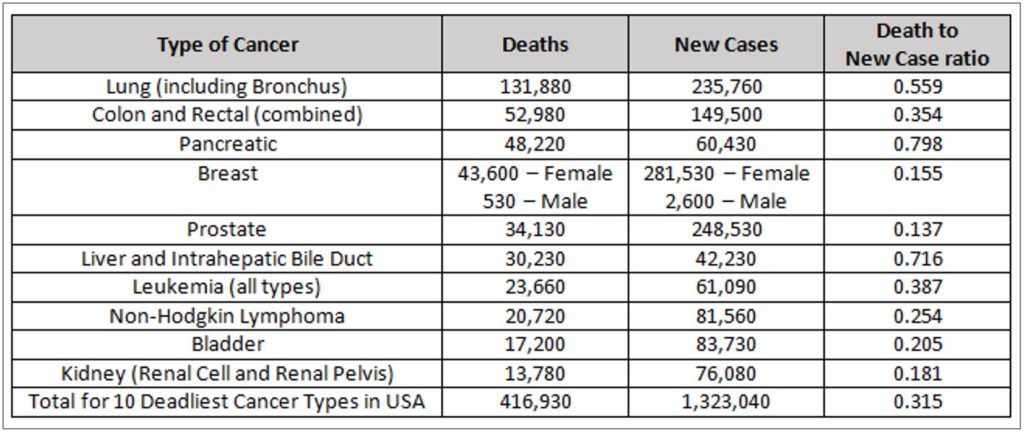
We have much to learn about preventing and treating cancer. Each disease in the cohort of cancers is potentially a different disease related to the specific genetic mutations that drive it. In the interest of promoting further efforts to improve our understanding of these complex diseases, here is an update on research involving three essential nutrients: vitamin C, selenium (selenite and methyl selenocysteine), and vitamin E (delta tocotrienol). Although much progress has been made in the fight against some types of cancer, many types still remain literally a death sentence. Each year, more than 1.3 million people are diagnosed with one of the ten most deadly types of cancer in the United States and over 400,000 people die from these dreaded diseases.
Ascorbic Acid (Vitamin C)

By definition, a vitamin is essential for life, and vitamin C (ascorbic acid) is no exception. The health benefits of vitamin C are so extensive that it would be an important tool in the battle against cancer even without its powerful anti-tumor effect. Vitamin C is important for many aspects of immune and endothelial health; synthesis of catecholamines, carnitine, neuropeptides, neurotransmitters, collagen, and elastin; breakdown of L-tyrosine and hypoxic inducible factor 1-alpha (HIF-1a); epigenomic regulation; somatic stem cell reprogramming; and redox regulation including scavenging damaging free radicals, breaking chains of lipid peroxidation, and recycling other antioxidants.2-8

In 1976, Cameron and Pauling reported longer survival in terminal cancer patients given vitamin C. 9 Was this from improvement to the patients’ constitution, was there an anti-tumor effect, or both? We now know that high doses of vitamin C can have a prooxidant effect, especially in combination with iron, which can selectively kill tumor cells containing less catalase than healthy human cells.10,11 The catalase enzyme is necessary for nearly all cells to remove hydrogen peroxide that can cause free radicals and damage the cell’s biomolecules, including proteins and DNA. And vitamin C can also disrupt the “Warburg Effect” in tumor cells.12,13,14 The Warburg Effect is the tendency of tumor cells to switch from using mitochondrial oxidative phosphorylation to aerobic glycolysis for the production of cellular energy (ATP). While greatly reducing the efficiency of energy production (2 ATP molecules generated per glucose molecule vs. 36 ATP molecules generated per glucose molecule), aerobic glycolysis enhances the ability of the cell to proliferate. Efficiency is only important when resources are scarce. In a glucose-rich environment, 2 ATP molecules per glucose will work just fine, and allows more of the glucose, along with the amino acid glutamine, to provide the structures necessary to make additional tumor cells. This primitive, yet streamlined, tumor metabolism allows abundantly available glucose and glutamine to supply the biochemical needs of cell growth and division. Many tumor cells over-express glucose transporters, particularly GLUT1 to increase intake of glucose. Ascorbic acid, and especially oxidized ascorbic acid (dehydroascorbic acid), is similar in molecular shape to glucose and can enter cells through these membrane transport channels. Not only does this disrupt the supply of glucose to the tumor cell, it also allows increased vitamin C concentrations within the cell where it can cause epigenetic effects including increasing TET enzyme activity, re-expression of tumor suppressor genes, or cause cell death through metabolic disruption. Depletion of intracellular glutathione leads to inactivation of glyceraldehyde 3-phosphate dehydrogenase and inhibition of glycolysis. In the setting of high vitamin C concentrations, the reliance of some tumor cells on aerobic glycolysis becomes their “Achilles’ heel.”15

In recent years, cell culture studies and human clinical trials have confirmed that tumor cells with KRAS and BRAF mutations can be selectively killed by appropriate doses of vitamin C.16 KRAS and BRAF mutations are common in solid tumors, especially pancreatic, colon, and lung cancers. Synergistic effects have been seen by combining vitamin C with some chemotherapy drugs, radiation treatment, or in combination with a fasting-mimicking diet.17-23 Mark Levine, Channing Paller, Tami Tamashiro, Thomas Luechtefeld and Amy Gravell recently reviewed 53 cancer clinical trials involving IV and/or oral vitamin C.15 These trials give a clear signal of safety when patients with glucose 6 phosphate dehydrogenase (G6PD) deficiency are excluded from high dose IVC administration. Most studies were small and involved a wide variety of late-stage cancers. Nonetheless, encouraging signals were seen, including a few patients surviving years later eventually dying of causes other than cancer. Studies involving pancreatic ductal adenocarcinoma (PDAC) show a median survival following diagnosis of 3.5 months untreated, 6.7 months when treated with gemcitabine, 8.5 – 13 months when treated with gemcitabine and nab-paclitaxel, and 15.1 months when IVC with or without gemcitabine was used.17,24 It is likely that with refinement of dosing and route of administration, earlier intervention, and improved knowledge of which tumors are most susceptible to high dose vitamin C therapy, more consistent positive results will be seen.
Three promising active clinical trials:

- A Phase II Trial of Pharmacological Ascorbate, Gemcitabine, and Nab-Paclitaxel for Metastatic Pancreatic Cancer (PACMAN 2.1; University of Iowa Holden Comprehensive Cancer Center)25
- A Phase II Study of High Dose Vitamin C Intravenous Infusion in Patients with Resectable or Metastatic Solid Tumor Malignancies (Weill Cornell Medicine, NYC)26
- To download an informative description of “IV Vitamin C for Cancer Care,” please click https://riordanclinic.org/wp-content/uploads/2017/09/IVChandout.pdf.
(Riordan Clinic, Kansas, >250,000 IVC treatments provided)27
Selenium
Selenium is a micronutrient essential for human health. There are 25 human selenoproteins known to be involved in numerous functions throughout the body, including brain, blood vessel, heart, and immune system health. These proteins perform diverse functions including antioxidant and redox recycling, gene “proof-reading,” vitamin D metabolism, and hemostasis. Like vitamin C, even if there were no direct tumor effect of selenium, it would be an important tool in the battle for wellness and against cancer.28-31
HLA-E is a “camouflage protein” expressed by some tumors to hide from the immune system. The protein fools the immune system into thinking the tumor cell is a normal cell. A decade ago, selenite was shown to reduce—nearly eliminate—HLA-E expression on tumor cells. The tumor cells then became susceptible to destruction by natural killer cells (immune cells which clear unhealthy cells from the body).32 A recent study of 243 PDAC patients showed that higher HLA-E and HLA-G (a similar protein) expression was associated with shorter survival.33 In addition to optimizing tissue health throughout the body, the reduction of camouflage membrane proteins HLA-E and HLA-G by selenite may be a useful tool in the battle against cancer. Of note, selenomethionine (SeMet) had no effect on tumor cell HLA-E expression. Selenomethionine was the form of selenium used in the SELECT trial which did not show a benefit of selenium against prostate cancer prevention. In addition to the unfortunate choice of selenium supplement, the trial had other flaws, including a lack of difference in selenium levels between the control and test groups. Methyl selenocysteine (MSC) was the form of selenium used in the Nutritional Prevention of Cancer (NPC) trial which showed benefit. MSC is also the dominant form of selenium in broccoli, cabbage, onions, and garlic. In 2014, MSC was shown to protect against the toxicity of four chemotherapy agents (cyclophosphamide, cisplatin, oxalplatin, and irinotecan), and enhance antitumor activity.34

More recently, a phase I study at Stanford using selenite and radiation therapy in humans validated the further study of selenite against cancer.35 Additionally, in vitro and in vivo (mice) studies at the University of Grenada showed a strong antitumor effect of selenite against pancreatic cancer, alone and in combination with gemcitabine.36
Delta Tocotrienol
Vitamin E is an essential nutrient for humans. Vitamin E is a lipid soluble antioxidant. There are eight different molecules in the vitamin E family pertinent to humans. It comprises four tocopherols (alpha, beta, gamma, delta), and four tocotrienols (alpha, beta, gamma, delta). Tocotreinols are smaller than tocopherols and are unsaturated. Tocotrienols have a half-life of approximately four hours while tocopherols have a half-life of 20 hours. Delta tocotrienol (VEDT = Vitamin E Delta Tocotrienol) is the smallest member of the vitamin E family, as it has the shortest “tail.” Its small size allows delta tocotrienol greater mobility within lipid layers of cell membranes.
Studies have shown that tocotrienols inhibit nuclear factor kappa B (NF-kB) activity and human pancreatic cancer cell survival, with VEDT having the strongest effect.37 NF-kB is involved in immune and inflammatory responses, and in the regulation of cellular gene expression, proliferation, differentiation, and survival. VEDT has also been shown to enhance gemcitabine activity in pancreatic cancer cells.38-40 Furthermore, VEDT has been shown to inhibit PDAC stem-like cells. VEDT significantly inhibited growth and metastases of these cells, including inhibiting the growth and metastasis of gemcitabine resistant PDAC stem-cell-like cells.41 A phase I human clinical trial at Moffitt Cancer Center in Tampa, Florida showed 200 to 1600 mg VEDT taken orally daily for two weeks was well tolerated and significantly induced apoptosis (cell death) in pancreatic ductal cancer cells.42 An anti-tumor effect, as well as a reduction in side effects from chemotherapy, has also been shown in the setting of other solid tumors.43-56
Note that to prevent the larger tocopherols from blocking absorption of the smaller tocotreinols, it is best to avoid taking tocopherols at the same time as tocotrienols. [57-63] Twice daily dosing of tocotrienols have been shown to produce a steady state after three days.
Summary

The redox synergy of vitamin C, vitamin E, and selenium-containing glutathione peroxidases has been explored since the 1960s and 1970s. Studies focusing on single nutrient interventions, with and without chemotherapy and radiation, have suggested benefit in humans, with increasingly specific mechanistic and treatment details discovered each decade. Along the way, a reassuring safety profile of nutrient interventions with and without traditional chemotherapy and radiation interventions has been established. Further studies to better define the most effective match of treatment for each tumor type, along with the best route, dose, and combination of treatments are important next steps to improve the reliability and effectiveness of preventing and treating the many types of cancer. Combining nutrients known to be synergistic together, while limiting glucose and glutamine central to the metabolism of many tumor cells, may optimize the effectiveness of treatment strategies.
With nutrient therapy—orthomolecular medicine—one does not need to choose between attacking the tumor and strengthening the host. The treatments often impact both simultaneously.
Foundational Support
- NAD deficiency is associated with greater risk for mutagenesis with cancer and this is likely best avoided using daily niacin, e.g. start with 3×25-100 mg/d to adapt to the flush, and then slowly work up to 3×500-1,000 mg/d.64 You can start by purchasing 100 mg tablets and break them into halves or quarters at first.
- For cancer patients, chemotherapy commonly causes NAD deficiency, which is best rescued with niacinamide; e.g. 3×500 mg/d.64
- Dietary relevance, glutamine restriction with niacinamide; glucose restriction and ketogenic diet is recommended.64
- Vitamin D3 to maintain plasma vitamin D >40 ng/ml. Test a dose of 125 mcg/d (5000 IU) D3 with 100 mcg/d K2 for four months before getting a blood test for vitamin D.
- 100-200 mcg/d selenium as methyl-selenocysteine or selenium yeast
- 300 mg/d alpha lipoic acid
- 1-2 g vitamin C with each meal
- Exercise
- Cultivate a cheerful heart65
Advanced Support
- Vitamin C in divided doses throughout the day to bowel tolerance; consider mixtures of lipid- and water-soluble forms
- IVC if G6PD levels are adequate and IVC is available from a licensed medical provider66
- Sodium selenite if available from a licensed medical provider
- Delta tocotrienol 300 – 1600 mg/d42
Michael Passwater is certified by the American Society for Clinical Pathology as a medical technologist, a specialist in immunohematology, and a diplomate in laboratory management. He has worked in clinical laboratories for 28 years and has his degree in medical technology from the University of Delaware.

Orthomolecular Medicine News Service free subscription link is http://orthomolecular.org/subscribe.html and the OMNS archive is http://orthomolecular.org/resources/omns/index.shtml.



