By Simon Yu, MD, COL, USA (Ret)

Dr. Tom Frieden, former director of the Centers for Disease Control and Prevention (CDC), opened up a new front in the coronavirus war by saying we don’t just need to treat the acute disease, we need to treat the underlying conditions that make people more susceptible to serious disease progression.1 He focused on heart disease and managing mitigating risk factors, such as CVD, diabetes, hypertension, and smoking in order to increase people’s odds for recovery. The initial focus has been pneumonia and acute respiratory distress syndrome (ARDS) with risk factors, including asthma, chronic obstructive pulmonary disease, and emphysema.
Dr. Frieden calls for better management of people’s underlying health problems to help mitigate the impact of COVID-19. I would take this one step further and say we need to go beyond managing chronic diseases and find and treat the pathogens that underlie and fuel their pathologies. Why?

In 2001, my work as an US Army Reserve medical officer took me to Bolivia to treat 10,000 Andes Indians with parasite medications. Not only did this resolve their parasite problems, but many reported it helped them overcome a range of additional chronic health problems. When I returned to St. Louis, I began to dig deeper with my chronic disease and “mystery disease” patients and treat some of them for parasite problems and saw many improve. I expanded this “search and destroy” mission with my patients to fungal and dental infections, as I learned many such infections—often overlooked in medicine today—are overlapping, synergistic, and can present as chronic illness.
The more I learned about the importance of a healthy biological terrain and the importance of a healthy immune system, the more I began to apply military thinking and strategy to medicine, and paradoxically, help the body find peace within itself. Sun Tzu wrote, “The supreme art of war is to subdue the enemy without fighting,” in his classic, The Art of War. I learned the best way to do that is strengthen the immune system, by focusing on such basics as nutrition, exercise, sleep, and emotional balance. When it comes to chronic illnesses, my belief is that we should not fight symptoms, a diagnosis or a syndrome, but improve the biological terrain, and counter the underlying asymmetric threats.
The importance of a multipronged effort to strengthen the immune system and treat the multiple pathogens that lead to an inflammatory cascade is underscored by new CDC data on COVID-19 in the US.2 Of 7,162 cases from mid-February to late March with complete information, the CDC found that 78 percent of people requiring admission to an intensive care unit (ICU) had at least one underlying health condition. Of people hospitalized but not requiring ICU admission, 71 percent had at least one such condition, compared with just 27 percent of people who didn’t need to be hospitalized. The biggest risk factors contributing to hospitalization and ICU admission were diabetes, lung disease, and CVD.2
In addition to preexisting heart, lung, and metabolic conditions, another major risk factor is an overactive immune system – a “cytokine storm.” According to Dr. Randy Cron of the University of Alabama at Birmingham, in as much as 15 percent of people battling any serious infection, “the immune system keeps raging long after the virus is no longer a threat. It continues to release cytokines that keep the body on an exhausting full alert. In their misguided bid to keep the body safe, these cytokines attack multiple organs, including the lungs and liver, and may eventually lead to death.”3 This may be the turning point from a mild to miserable respiratory illness into life-threatening organ failure.
| Underlying health condition/ Risk factor for severe outcomes | Not hospitalized | Hospitalized, non-ICU | ICU admission | Hospitalization status unknown |
| (top three conditions listed below) | (number, percent with condition) | |||
| Total w/ complete information (7,162) | 5,143 | 1,037 | 457 | 525 |
| One or more conditions (2,692, 38%) | 1,388 (27%) | 732 (71%) | 358 (78%) | 214 (41%) |
| Diabetes mellitus (784, 11%) | 331 (6%) | 251 (24%) | 148 (32%) | 54 (10%) |
| Chronic lung disease (656, 9%) | 363 (7%) | 152 (15%) | 94 (21%) | 47 (9%) |
| Cardiovascular disease (647, 9%) | 239 (5%) | 242 (23%) | 132 (29%) | 34 (6%) |
Source: http://dx.doi.org/10.15585/mmwr.mm6913e2
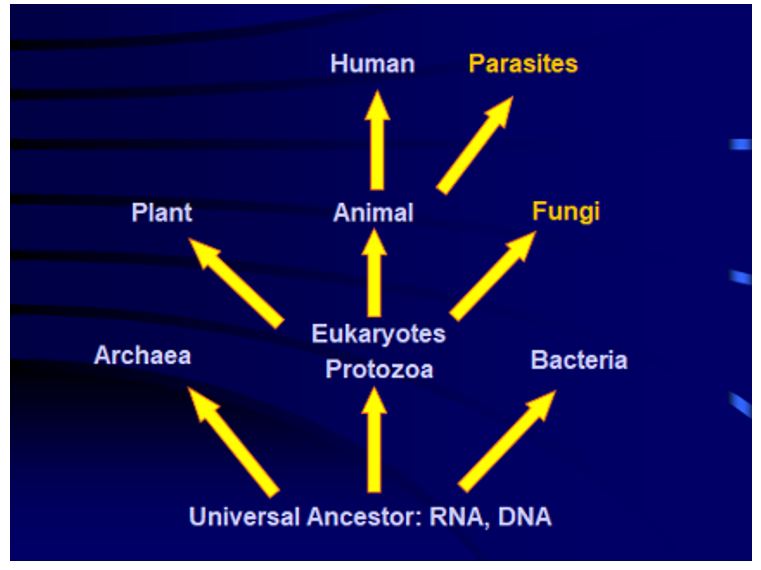
What have I learned in my years of medical practice as a regional HMO director, 25 years in the US Army Reserve Medical Corps, and as director of Prevention and Healing, Inc. in St. Louis? The asymmetric threats most often overlooked are parasites, fungal infections, and dental problems. Viruses are technically parasites, a gray area between living and nonliving: they cannot replicate on their own but do so in living cells. They have been evolving with us and some of them are encoded as a part of our genetic code from the point of evolution of biological life. They are unique and complex, composed of a protein coat surrounding RNA or DNA core genetic materials. They can stay dormant for many years or be active seasonally and are capable of growth and multiplication only in living cells as unwanted guests, just like parasites. Parasites have their own parasites, fungi, mycoplasma, bacteria, and many types of viruses. The slide below is part of my lecture explaining the evolution of life and parasites, coinfections and parasitic relationships from a universal, simplified perspective.
The coronavirus is deceptive and creates a hidden chain reaction. COVID-19 will attack aggressively already vulnerable aging populations and immune-compromised, chronically ill patients, young or old. Many patients are nutritionally depleted and cannot support their immune system, so rapidly succumb to the viral infection. By the time one develops pneumonia, COVID-19 may activate dormant, inactivated bacteria, fungi, mycobacteria, and parasites that were previously under the surveillance of the immune system. COVID-19 pneumonia patients may be fighting more than viral infection but also bacterial, mycobacterium-TB-like infection, fungi and reactivated parasites, including dental infections. Prevotella have been found in lungs of COVID patients in three Asian studies; it is often found in dental infections.4

Coinfections might explain why some patients respond to hydroxychloroquine, an antimalarial parasite medication, and azithromycin, an antibiotic for pneumonia, one of numerous treatment strategies now being tested. Hydroxychloroquine facilitates uptake of zinc into cells, which interrupts viral replication.5 Another repurposed medication being tested is losartan, an angiotensin-converting enzyme (ACE) inhibitor blood pressure medication. ACE-2 is the host cell receptor responsible for mediating infection by SARS-CoV-2, the novel coronavirus responsible for coronavirus disease 2019 (COVID-19). Treatment with anti-ACE-2 antibodies disrupts the interaction between virus and receptor.6
Physicians in Shanghai report help from using high and frequent dose IV vitamin C.7 A clinical trial using vitamin C for coronavirus is underway in China,8 and it is also in use in some New York City hospitals.9 While pharma companies are eager to fund trials of costly patented drugs, we also need to test combinations of existing drugs and nutrients to find more accessible, affordable solutions.

For prevention and prophylactic measures, I recommend extra vitamin C up to 10,000 mg/day, 10,000 IU of vitamin D3, vitamin K2, selenium, zinc, boron, and herbal and homeopathic remedies for viral respiratory illnesses, such as elderberry extract. Glutathione can be used for general immune support. I am not saying this will prevent or stop COVID-19, but help you be in a stronger position to fight it.
In the face of the coronavirus pandemic ravaging the US, the FDA has rapidly issued a series of Emergency Use Authorization (EUA) Updates for Coronavirus Disease (COVID-19), which cover in vitro diagnostic products, personal protective equipment, other medical devices, and therapeutics.10 In addition, FDA approved two new treatments being used overseas in late March: convalescent plasma therapy, and hydroxychloroquine, an antiparasitic used for malaria, lupus, and rheumatoid arthritis. Both of these have a long history of successful use for other diseases: side effects are understood and should be monitored; and clinical trials are being initiated.
The Food and Drug Administration (FDA) has created a special emergency program for possible therapies, the Coronavirus Treatment Acceleration Program (CTAP).11 As of this writing, there are 10 therapeutic agents in active trials, and another 15 in planning stages. FDA invites new requests for product development for proposed COVID-19 uses and drug development submissions at COVID19-productdevelopment@fda.hhs.gov.
There is a good deal of controversy in medical circles about whether the FDA is moving too fast, or too slowly, in clinical trials and drug approval. Given the gravity of the challenges we face, it is time to put aside intellectual biases and be open to new strategies. It is time for “all hands on deck.”
Just as public health strategies of isolation, quarantine, and containment play a vital role in pandemics—in addition to emergency medicine and targeted therapeutics—there is an important role for preventive and integrative medicine. We need to treat the whole body and strengthen the biological terrain to be ready to confront both novel viruses and longstanding pathogens that contest for living among, within, and off of us. We need extra help in the face of the asymmetric threats we confront in the challenging months ahead in our families, our nation, and our stressed and overstretched healthcare system.
Simon Yu, MD, Col (Ret), practices internal and integrative medicine at Prevention and Healing, Inc. in St. Louis; his latest book is AcciDental Blow Up in Medicine: Battle Plan for Your Life.
References

1. Frieden T. Former CDC Chief Dr. Tom Frieden: Coronavirus and cardiovascular disease – stopping a deadly disease. Fox News. March 25, 2020.
2. Centers for Disease Control and Prevention. Preliminary Estimates of the Prevalence of Selected Underlying Health Conditions Among Patients with Coronavirus Disease 2019 — United States, February 12–March 28, 2020. MMWR. April 3, 2020.
3. Mandavilli A. The coronavirus patients betrayed by their own immune systems. The New York Times. April 1, 2020.
4. Chakraborty S. SARS-Cov2 enables anaerobic bacteria (Prevotella, et al) to colonize the lungs disrupting homeostasis – symptoms (ARDS, septic shock, blood clots, arterial stroke) finds resonance, with key differences, in the ‘forgotten disease’ Lemierre Syndrome, caused by anaerobic bacteria enabled by Epstein Barr Virus. OSF Preprints. February 3, 2020.

5. Gautam CS, et al. Potential Armamentarium to Contain COVID-19 Pandemic in Developing Countries: Be Prepared and Act Timely! ACTA Scientific Paediatrics. April 4, 2020.
6. Fang L, Karakiulakis G, Roth M. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? The Lancet. April 2020.
7. Lichtenstein K. Can Vitamin C prevent and treat coronavirus? MedicineNet. March 9, 2020.
8. Vitamin C infusion for the Treatment of Severe 2019-nCoV Infected Pneumonia. ClinicalTrials.gov. ClinicalTrials.gov Identifier: NCT04264533
9. McCall R. New York Hospitals Are Using Vitamin C to Treat Some Coronavirus Patients. Newsweek. March 26, 2020.
10. US FDA. Emergency Use Authorization.
11. US FDA. Coronavirus Treatment Acceleration Program.



