by Sangeeta Pati, MD, and John Apsley, MD(E), ND, DC

In the 1990s when I (SP) was in medical school, I had not heard of the term “fibromyalgia.” As a matter of fact, this condition came directly into my consciousness only after I started to practice regenerative medicine. That’s when patient after patient started coming through my door with “fibromyalgia”: fatigue and pain of unknown origin. They were looking for a way to treat their condition that differed from conventional medical practice. Many had been placed on pharmaceutical products intended to “give them their life back.” Yet these patients almost always lost much of their ability to function. In fact, many of them were on full disability. It became clear that we were not treating root causes.

Over the years, the quest for the root causes for fibromyalgia led to an understanding that they are no different from the root causes of all chronic conditions. Regenerative medicine starts with determining true causation and then restoring and rebalancing the body by tapping into the innate healing powers found in every living being. This customized approach to healing is a system that enables the body to regenerate itself. We define regeneration as unscheduled healing, that is, healing unlikely to take place with conventional approaches.
In this article, we share some insights from our Regenerative Protocols That Work™ that we have used to successfully address root causes in thousands of patients. This includes the physicians or their family members (>20%) that seek our care and learn these methods from our workshops. Chronically ill patients who adopt this regenerative model achieve a full recovery over 85% of the time. Additionally, we are even more fortunate in that when our patients consistently stick to their full program, they enjoy a much lower risk of acquiring future chronic diseases, including cancer, than the national averages.
How Joan Got Her Life Back

Joan, age 54, arrived on my doorstep in 2005 with debilitating pain. Despite a plethora of pain medications and Lyrica, she was unable to function at even a basic level and reported long-term disability. At that time, I was just getting my feet wet in the world of integrative medicine. As an Ob/Gyn, I started with bio-identical hormone therapy – some estrogen, progesterone, and testosterone. In four weeks, she returned for a follow up visit and reported, “My pain is a little better. I’m sleeping better, and I want to go all the way.” It was Joan, and then hundreds of patients after her who motivated the journey and a framework that became the foundation for our five-point regenerative model. This causal approach (i.e. 5-point model system described below) has been specifically utilized to empower every patient to be “in the driver’s seat for their own recovery.” A key concept is the ability to wean patients off of outside influences and medications, gradually moving them towards their innate state of optimal health and homeostasis. I still see Joan today. She remains off all medications, remains pain-free, and has sustained, vibrant energy. In a phrase, Joan got her life back!
The Best Model for Regeneration
In 2017, we had the blessing of having Dr. John Apsley, author of the Regeneration Effect series, consult in our practice. With over 40 years of research, he had identified the precise means by which long-living people implement a daily regenerative lifestyle to thrive. By adding his advanced regenerative methodology to our practice, patients are more quickly enabled to become the primary driver to their own recovery. This is critical to the many patients who are long disempowered to even think recovery is possible due to chronic illnesses. A regenerative lifestyle is all about addressing the causations to how the long-living thrive. So, our clinic providers are able to manage even more difficult cases, more cost-effectively because we do not have to chase after so many of the down-stream complexities that are now so inherent to chronic cases.

For example, in the literature one finds a myriad of possible causes of fibromyalgia, including physical inactivity,1 autoimmunity, infections,2 parasites, toxins, heavy metals, vaccines, dysbiosis, nutritional deficits, adrenal insufficiency, mental abuse, depression3 and chronic stress.4 Chasing any one of these causes never results in a complete, sustainable cure because these are downstream from the basic factors that control the internal environment. Here, we can learn from the long-living cultures who are regenerating in the Blue-Zones (Figure 1, above). Around the world there are well-studied zones, where people live long healthy lives, climbing mountains, herding goats and flourishing until they are above 100 years old.5-7 These people experience aging biomarkers at the cell-level after an age of over 80.8-11 In the US, although some small improvements are being seen in our young from two decades ago (e.g., metabolic syndrome), the onset of deadly chronic degenerative diseases and aging biomarkers begins in our teens. In our adult population, cancer rates, cardiovascular disease, chronic kidney disease, obesity and diabetes are soaring.12 What is the secret of the long-living? Is it the food? Is it the water/the soil? Is it the lifestyle? Is it the purpose and joy? Only over the past decade have we begun to understand the critical components of that Regeneration Effect, components that can be applied in a customized fashion to reverse chronic conditions and keep us happy, healthy, and free of dis-ease.

Treat the Clinical Picture, Not the Lab
At the University of Maryland in 1990, Dr. Frank Calia spoke: “Treat the patient, not the lab.” The truth of that lesson only became crystal clear after I entered this field and realized that most of the patients with debilitating symptoms still had lab parameters in the “normal range.” When we measure levels through the lab, we are measuring only one fraction of what actually constitutes “function.” So, an active thyroid level (free T3) tells us what is circulating in the serum. The factors that affect its function, however, include the receptor-site sensitivity, co-factors like selenium and zinc, and tissue pH. This is the classic patient who has all the thyroid symptoms and are told they are normal. So, one cannot rely on the thyroid serum levels alone; we have learned that the clinical picture generally supersedes the lab.
Chronic Illnesses reverse as patients begin to thrive and experience joy.
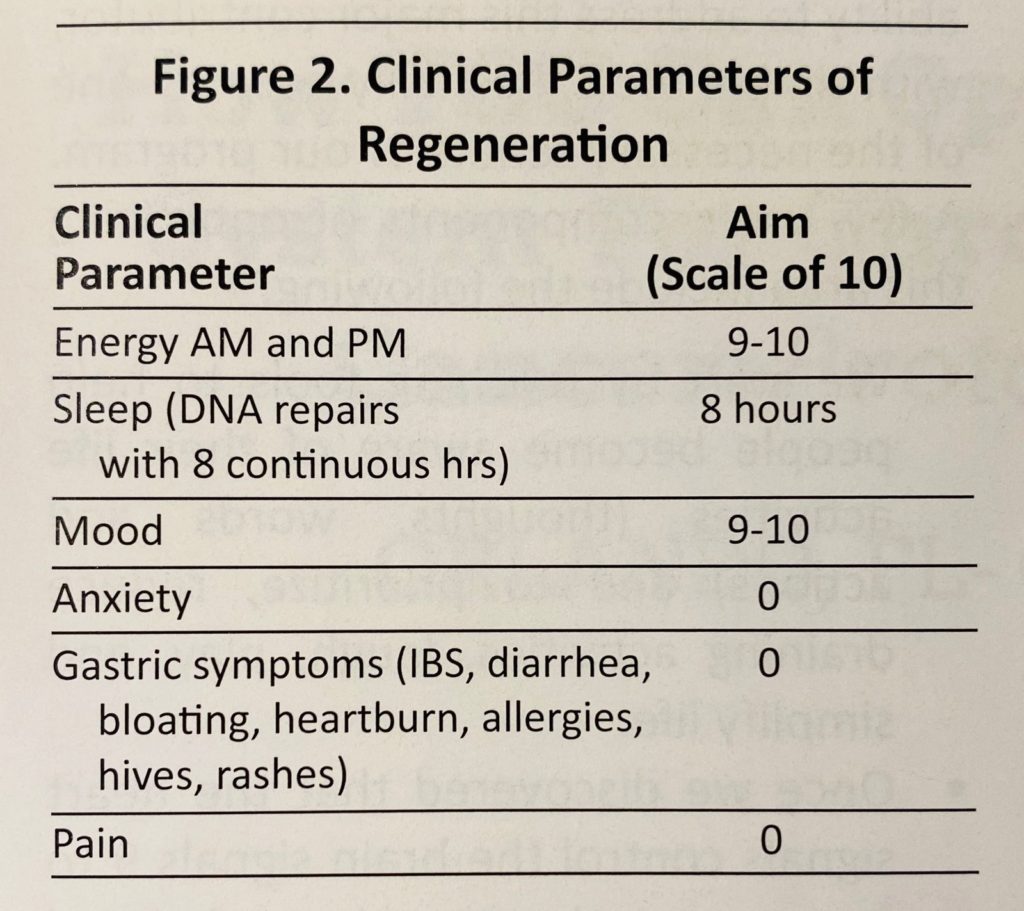
Over time we learned that regardless of the condition, when the patient truly “feels like they’re thriving,” regeneration is occurring and chronic disease is reversing. Specifically, when a person experiences vibrant energy, restorative sleep, tranquility, joy, a healthy gut, and is pain-free, they are regenerating. Our experience in tens of thousands of patients is that these six clinical parameters of regeneration correlate with reversal of chronic disease. We follow and correct these parameters in every patient at every visit (Figure 2, below).
Lab Measurement
Although, the clinical picture is primary, we follow labs for general guidance and safety. Which route and which levels?
First, we’ll briefly address the conundrum of whether one looks at serum, saliva, or urine for hormones. The serum level tells us what is circulating. The salivary level tells us what is in the tissue. The urine gives us the metabolites. We started this journey in 2005 by measuring all three sources. We realized that we were basing our therapies and dosing primarily on the clinical picture as explained above; so whichever source we used, it was reasonable as long as we knew how to interpret it to address and safely coax the body back to optimal health. They provide three different pieces of information. One is not better than the other.
“Optimal” levels are different from “normal” levels. “Optimal” is defined by the upper quartile where the literature supports protective effects. We are not aiming for “normal” levels between the 5th and 95th percentile. We are aiming for the quartile in the direction of health: greater than 75th percentile for hormones and nutrients, and less than 25th percentile for sugars and cholesterols. For example, we aim for the 25-hydroxy vitamin D to be above 70 ng/mL, although the “normal” range is 30-100 ng/mL. This level is where the thyroid and metabolism function best and where maximum protection from immune failure, cancer, strokes and heart attacks lies. We are aiming for a full tank of steroid hormones (>75th percentile) in the morning, as this is where the body is optimally protected from disease. So, we aim for a DHEA-S above 200 ug/dL, whereas the “normal” range is 45-440 ug/dL. We aim for a pregnenolone above 150 ng/dL. The “normal” range is 0-237 ng/dL. Imagine waking up at a level of zero and being told that that is “normal.” We aim for a free T3 above 4.5 pg/mL (normal range is 2.3-6.8 pg/mL). This is where the patient is clinically optimal. Let’s see how this is applied to patients.

The Five Point Model System to Regenerative Medicine
There are five basic, foundational areas that need to be optimized in order to produce a regeneration effect at the DNA level that will reverse any condition, including fibromyalgia. Together, they comprise our Regenerative Protocols That Work™. These areas are 1) mind/heart,13-15 2) body,16-18 3) hormones,19-21 4) nutrition,22-24 and 5) detoxification25-27 (Figure 3).

for Regenerative Protocols That Work™
When these five basic, foundation areas are optimized and coordinated, it replicates the factors causing the people of the Blue-Zones to thrive. For illustration, the long-living folks in the Blue-Zones connect themselves to everyone and everything around them through 1) joy, 2) oxygen, 3) sunlight, 4) earth/soil, and 5) structured water (Figure 3). When practiced all together and concomitantly, our Regenerative Protocols That Work™ are created, which in turn facilitate each patient to enter “the driver’s seat to their recovery” and feel their life is thriving.
So, what is this basic framework utilized to empower every patient to be “in the driver’s seat for their own recovery?” First, it is critical that patients have a Regenerative Health Coach for 90 days who works with them closely to master the protocols that comprise the five-point model system:
Mind/Heart stress is the base of all chronic disease. The easiest way to gauge this is to assess whether JOY is present or not. If joy and purpose are not present, the body has no reason to stick around. One can think of mind stress as those stressors that are in our consciousness like relationships, finance, health, and hope. These account for about 10% of what affects our body. Then there is the heart stress or emotional stressors, which can account for approximately 90% and can often be in our subconscious, so we need to address both.

It is not necessarily the occurrence of stressful events and emotions in life that creates dis-ease. It is the way in which we respond to these events. We cannot change a hurricane; we can alter the way in which we respond to the hurricane and the impact it has on our physical body. When the response is sustained, we are in an inflammatory chronic stress response.28-30 Here, the “fuel tank” of hormones and nutrients is depleted. Here, the message to the body is not one of hope. There is not one patient with “fibromyalgia” who does not have the chronic stress response as a major contributor. The ability to address this major contributor, with simple tools, has truly become one of the necessary tenets of our program. A few main components of optimizing this area include the following:
• We start by teaching tools to help people become aware of their life activities (thoughts, words and actions) and to prioritize, reduce draining activities, laugh, play, and simplify life.
• Once we discovered that the heart signals control the brain signals 9 to 1; we started to use heart-focused meditation, which can convert the nervous system in 30 seconds. We ask every patient to utilize Heart-Math Institute’s heart rate variability (HRV) application (i.e. InnerBalance App) and aim for a “coherent heart rhythm” for five minutes twice a day, through creating a feeling of joy.31,32 The effects lasts for hours (Figure 4, below).
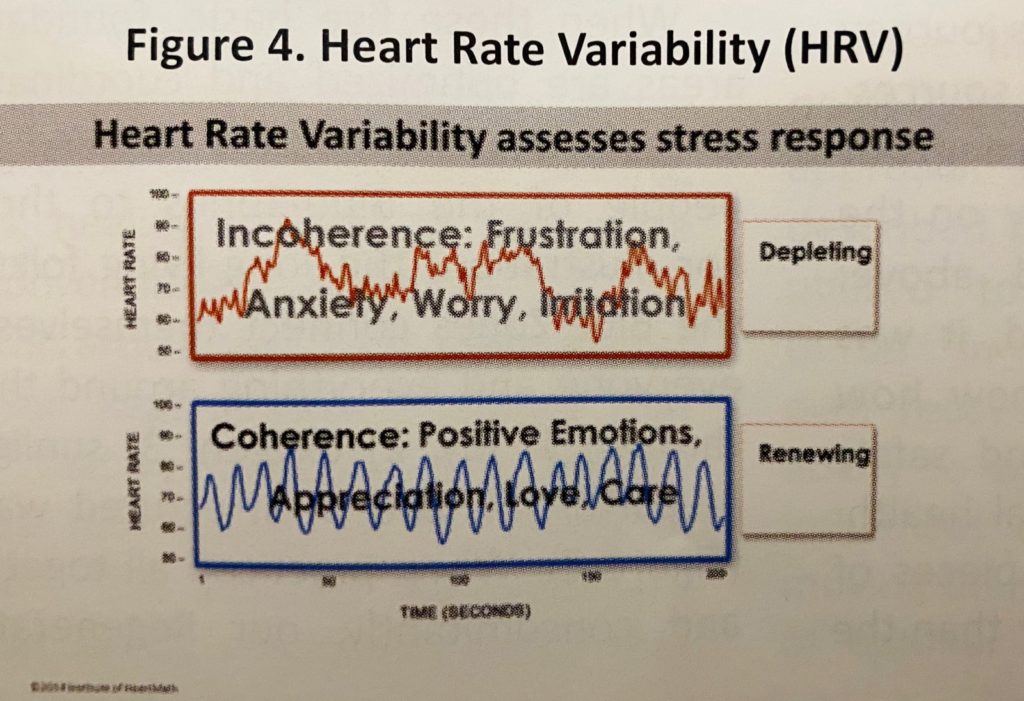
• In a “coherent state”, the patient must state their affirmation to fully recover with vibrant energy and a pain-free life. Often the subconscious program or belief in chronically ill patients is a major source of continued illness. As we know the heart to be the strongest electromagnetic field in the body, the vibration created by HRV helps to program the water structure in the body and around the DNA, either with a full recovery or with incoherence and continued dis-ease.
Note that as we have become aware that the gut impacts 70% of the nervous system,33-35 we have correlated incoherent heart rate variabilities with gastric inflammation, which is a component in every chronic disease including fibromyalgia. Gut imbalances present in a variety of ways including IBS, colitis, autoimmunity, bloating, and leaky gut syndrome.
Body stress is ultimately related to the level of oxygenation in the small vessels. The physical body stressors are gauged by the level of pain and the level of physical activity. When pain and physical activity are high, the “fuel tank” of hormones and nutrients is being depleted and oxygenation to organs is low. By mass, oxygen accounts for about 65% of the human body,36 so improving oxygenation to the cell level is an essential part of every program. A few main components of optimizing this area include the following:
• Reducing physical activity where heart rate is above 120 beats per minute. Replacing that with oxygenating restorative exercise, such as yoga, tai chi, qi gong, stretching, gentle walks.
• Using techniques of conscious breathing such as pranayama and alternate nostril breathing.

• Using oxygen concentrators to deliver 98% oxygen during exercise (as opposed to lesser percentages, i.e., 30% to 70%, of inspired oxygen).37 High-Intensity Interval Training or HIIT with hyperoxia (e.g., Exercise With Oxygen Therapy – EWOT)38 is significantly superior than HIIT without hyperoxia.39-44
• Epsom salt baths with six to eight pounds of Epsom salts or one to two pounds of magnesium chloride flakes. This helps with magnesium, which is a mainstay.
• Aggressively reducing pain with anti-inflammatory agents such as liposomal curcumin, palmitoylethanolamide (PEA) and cannabinol derivatives (CBD). Reducing pain also occurs with the aggressive correction of cortisol pathway depletions (such as progesterone, DHEA, testosterone and cortisol) and nutritional deficiencies (such as high dose fish oil, lipid-soluble magnesium). The pain has got to go along with the medications used to control pain.
Hormonal imbalances are centered around insufficiency in adrenal and thyroid function. As discussed, every fibromyalgia patient has a chronic stress response that depletes the “fuel tank” of hormones and nutrients. While we are addressing the chronic stress response, we must “optimize” the fuel tank, including the adrenal and thyroid levels. We use serum levels as they are covered by insurance, defensible as the medical standard, correlate with published protective levels, and are convenient for the patient. Most importantly, we have learned how to interpret the levels properly in order to get the maximum results. Hormone imbalances are quite straightforward to correct when one uses a natural order of correcting the adrenal imbalances and then the thyroid. Only bioidentical hormones are used. A few main components of optimizing this area include the following:
• Whether male or female, we start with oral progesterone to calm down the nervous system and the HRV. We titrate this until the patient is sleeping for a solid, restorative eight hours without interruption.
• We optimize (>75th percentile) DHEA-S, testosterone, and pregneno-lone. Often, we use a short course (less than 6 months) of up to 40 mg of oral cortisol to break the cycle.
• We optimize thyroid until symptoms are resolved. These include fatigue, brain fog, depression, weight gain, constipation, skin dryness, and even pain.
Most patients eventually dial back their doses and even discontinue many hormones once they master optimizing their lifestyle. As they lower the “speed of the engine,” such as mental and physical stressors, they need less fuel.
Nutritional imbalances always accompany hormonal imbalances. When the “speed of the engine” is high over a prolonged period, the fuel tank gets depleted and nutritional levels fall below the 75th percentile, as we have learned through thousands of Spectracell™ micronutrient tests. A few main components of optimizing this area follow:
• The mainstay of the program is to optimize dietary food intake. We recommend organic food in a balanced plate ratio of 50% vegetables, 25% lean protein, and 25% complex carbohydrates.
• Eliminate all inflammatory foods like dairy and sometimes meat and fish.
• When using supplements, we aim for the least number of vegetarian capsules with no dyes, preservatives, fillers, or magnesium stearate.
• In addition to correcting measured deficiencies, there are four core supplements that these patients must have including magnesium (acetyl-taurinate) up to 1000 mg (depending on bowel tolerance), high dose fish oil (enteric coated), essential minerals and vitamins (for the adrenal/ thyroid axis), and probiotics.
We use nutritional intravenous therapies in the first two months as needed to accelerate results.
Detoxification aims at correcting water intake and pH. We have learned that identifying and addressing specific toxins through measurement is to be done only after the patient feels better because chasing toxins when a patient is feeling ill usually leads to further deterioration. Still we always start with detoxification basics, which address over 75% of toxins. A few main components of optimizing this area include the following:

• Drinking clean, structured water at least 100 ounces per day with pink salt and lemon. Water molecules comprise over 98% of all other molecules in human cells.45 Studies in the 1800s actually show reversal of chronic disease with adequate water intake.
• Monitor AM urine pH. Aim for >6.7. With proper hydration and alkaline pH, the toxic acids and xenobiotics stored in the body fat are automatically eliminated, often returning optimal immune functions.46-48
• Addressing the lining of the gastrointestinal system is critical in these patients. If there are gastric symptoms, we use a protocol with broad spectrum probiotics and enzymes. Sometimes we add glutamine and aloe, if we have evidence of significant gastric in-flammation. Turns out most patients do have this.
• Once the patient is feeling better, usually after the first 90 days, we address kidneys, liver, gallbladder, skin, and lymphatics.
Lastly and critically, it has become clear that every chronic condition is associated with a degree of immune compromise and insidious chronic infection, including chronic periodontal disease and chronically infected root canal teeth. So, we have had to perfect identifying and treating these through various diagnostics including muscle testing and combinations of hydrosol silver, ozone, and anti-infectives.
Conclusion
It is very encouraging to realize that all chronic conditions are treatable by addressing underlying root causes that also control our self-healing gene expression. When faced with a chronic condition like fibromyalgia, one must empower the patient’s self-healing mechanisms to take the driver’s seat for a complete cure. Our role as doctors is to provide awareness, hope, and tools that work. The effectiveness of tools and protocols is dependent on their simplicity aiming at the least steps and fewest capsules, so that the patient is not overwhelmed. When we can accomplish this, it is common to get tangible results within 90 days. Over time we have learned that regardless of the condition, when the patient truly begins to thrive, regeneration has been optimized, and their dis-ease is reversing. The defining elements to thriving are when a person experiences 1) vibrant energy, 2) restorative sleep, 3) tranquility, 4) joy, 5) a healthy gut, and 6) becomes pain-free (Figure 2).
Consider the five areas in the five-point model (Figure 3) as the “environment” or milieu that controls our genes (epigenetics). The most important component of this is the vibration of JOY that structures the water surrounding our DNA. This instantly initiates the receding of our inflammatory state. We would not be exaggerating if we expanded the message of the Beatles “All You Need Is Love” and concluded that “All You Need Is Joy.”
References
1. Booth FW, Roberts CK, Laye MJ. Lack of Exercise is a Major Cause of Chronic Diseases. Compr Physiol. 2012 Apr;2(2): 1143-1211.
2. Tan AC, et al. Chronic Widespread Pain and Fibromyalgia Syndrome: Life-Course Risk Markers in Young People. Pain Res Manag. 2019;2019:6584753.
3. Tan AC, et al. Chronic Widespread Pain and Fibromyalgia Syndrome: Life-Course Risk Markers in Young People. Pain Res Manag. 2019;2019:6584753.

4. Chu L, et al. Onset Patterns and Course of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Front Pediatr. 2019;7:12.
5. Buettner D. The Blue Zones: Lessons for Living Longer from the People Who’ve Lived the Longest. Washington DC: National Geographic; 2008. ISBN: 978-1-4262-0400-5.
6. McCarrison, R. Studies in Deficiency Disease. Milwaukee, Wisconsin; Lee Foundation for Nutritional Research; 1945.
7. Pitskhelauri, GZ. The Longliving of Soviet Georgia. Translated and edited by Gari Lesnoff-Caravaglia, New York, NY: Human Sciences Press, Inc.; 1982. ISBN-10: 0898850738; ISBN-13: 978-0898850734.
8. Panagiotakos DB, et al. Sociodemographic and Lifestyle Statistics of Oldest People (>80 years) Living in Ikaria Island: The Ikaria Study. Cardiol Res Pract. 2011 Feb 24;2011:679187.
9. Willcox BJ, Willcox DC, Suzuki M. Demographic, phenotypic, and genetic characteristics of centenarians in Okinawa and Japan: Part 1-centenarians in Okinawa. Mech Ageing Dev. 2017 Jul;165(Pt B):75-79.
10. Chrysohoou C, et al. Long-term fish intake preserves kidney function in elderly individuals: the Ikaria study. J Ren Nutr. 2013 Jul;23(4):e75-82.
11. Price W. Nutrition and Physical Degeneration. Price Pottenger Foundation (Editor). Price Pottenger Nutrition. 8th Edition. 2008. ISBN-10: 0916764206; ISBN-13: 978-0916764203.
12. AHA. Heart Disease and Stroke Statistics – 2017 Update: A Report From the American Heart Association. Circulation. 2017 Mar 7;135(10): e146-e403.
13. Wolf EJ, et al. The Goddess Who Spins the Thread of Life: Klotho, Psychiatric Stress, and Accelerated Aging. Brain Behav Immun. 2019 Aug;80:193-203.
14. Fastame MC, Penna MP, Hitchcott PK. Psychological markers of longevity in Sardinian centenarians: the impact of developmental factors and social desirability. Aging Clin Exp Res. 2019 Mar 13.
15. Wang J, Um P, Dickerman BA, Liu J. Zinc, Magnesium, Selenium and Depression: A Review of the Evidence, Potential Mechanisms and Implications. Nutrients. 2018 May 9;10(5). pii: E584.
16. Mok A, et al. Physical Activity Trajectories and Mortality: Population Based Cohort Study. BMJ. 2019 Jun 26:365:I2323.
17. Booth FW, et al. Role of Inactivity in Chronic Diseases: Evolutionary Insight and Pathophysiological Mechanisms. Physiol Rev. 2017 Oct 1;97(4):1351-1402.
18. Amaro-Gahete FJ, et al. Exercise training increases the S-Klotho plasma levels in sedentary middle-aged adults: A randomised controlled trial. The FIT-AGEING study. J Sports Sci. 2019 Jun 4:1-9.
19. Calabrese V, et al. Sex Hormonal Regulation and Hormesis in Aging and Longevity: Role of Vitagenes. J Cell Commun Signal. 2014 Dec;8(4):369-84.
20. Mora M, et al. Metabolic and Hormonal Contributors to Survival in the Participants of the Mataro Ageing Study at 8 Years Follow-Up. Clin Endocrinol (Oxf). 2014 Nov;81(5):775-83
21. Aoki Y, Aoki M, Yamada K. Leukocyte Telomere Length and Serum Levels of High-Molecular-Weight Adiponectin and Dehydroepiandrosterone-Sulfate Could Reflect Distinct Aspects of Longevity in Japanese Centenarians. Gerontol Geriatr Med. 2017 Mar 8;3:2333721417696672.
22. Cherif H, et al. Curcumin and o-Vanillin Exhibit Evidence of Senolytic Activity in Human IVD Cells In Vitro. J Clin Med. 2019 Apr;8(4):433.
23. DiNicolantonio JJ, O’Keefe JH, Wilson W. Subclinical Magnesium Deficiency: A Principal Driver of Cardiovascular Disease and a Public Health Crises. Open Heart. 2018;5(1):e000668.
24. Zhu Y, et al. New agents that target senescent cells: the flavone, fisetin, and the BCL-XL inhibitors, A1331852 and A1155463. Aging (Albany NY). 2017 Mar 8; 9(3):955-963.
25. Gadecka A, Bielak-Zmijewska A. Slowing Down Ageing: The Role of Nutrients and Microbiota in Modulation of the Epigenome. Nutrients. 2019;11:1251.
26. Martucci M, et al. Mediterranean Diet and Inflammaging within the Hormesis Paradigm. Nutr Rev. 2017 Jun 1;75(6):442-455.
27. Salah A. Sheweita, Editor. Biotransformation Profiles from a Cohort of Chronic Fatigue Women in Response to a Hepatic Detoxification Challenge. PLoS One. 2019;14(5). e0216298.
28. Hammadah M, et al. Inflammatory Response to Mental Stress and Mental Stress Induced Myocardial Ischemia. Brain Behav Immun. 2018 Feb; 68: 90–97.
29. Kerster A, et al. Corticosteroid signaling at the brain-immune interface impedes coping with severe psychological stress. Sci Adv. 2019 May; 5(5): eaav4111.
30. Boer AC, et al. Does psychological stress in patients with clinically suspect arthralgia associate with subclinical inflammation and progression to inflammatory arthritis? Arthritis Res Ther. 2018; 20: 93.
31. See https://www.heartmath.com/science/
32. Valderas Yamuza MT, et al. Human Emotion Characterization by Heart Rate Variability Analysis Guided by Respiration. IEEE J Biomed Health Inform. 2019 Jan 28..
33. Catanzaro R, et al. The gut microbiota and its correlations with the central nervous system disorders. Panminerva Med. 2015 Sep; 57(3):127-43.
34. Novotný M, Klimova B, Valis M. Microbiome and Cognitive Impairment: Can Any Diets Influence Learning Processes in a Positive Way? Front Aging Neurosci. 2019 Jun 28;11:170.
35. Natale G, et al. The nature of catecholamine-containing neurons in the enteric nervous system in relationship with organogenesis, normal human anatomy and neurodegeneration. Arch Ital Biol. 2017 Sep 1;155(3):118-130.
36. See https://en.wikipedia.org/wiki/Composition_of_the_human_body
37. Cardinale DA, et al. Influence of Hyperoxic-Supplemented High-Intensity Interval Training on Hemotological and Muscle Mitochondrial Adaptation in Trained Cyclists. Front Physiol. 2019; 10: 730.
38. Ardenne MV. Oxygen Multistep Therapy: Physiological and Technical Foundations. 1st Edition. Thieme. 1990. ISBN-13: 978-3137435013. ISBN-10: 3137435013
39. Kon M, Nakagi K, Ebi Y. Effects of All-Out Sprint Interval Training Under Hyperoxia on Exercise Performance. Physiol Rep. 2019 Jul;7(14):e14194.
40. Mallette MM, Stewart DG, Cheung SS. The Effects of Hyperoxia on Sea-Level Exercise Performance, Training, and Recovery: A Meta-Analysis. Sports Med. 2018 Jan; 48(1):153-175.
41. Ulrich S, et al. Mechanisms of Improved Exercise Performance under Hyperoxia. Respiration. 2017;93(2):90-98.
42. Hatfield SM, et al. Immunological mechanisms of the antitumor effects of supplemental oxygenation. Sci Transl Med. 2015 Mar 4;7(277):277ra30.
43. Freitag N, et al. A systematic review and meta-analysis about the effects of high-intensity interval training on physical fitness, health parameters and patient-reported outcomes in cancer survivors. German Sport University Cologne, Cologne, Germany. J Cancer Surviv. 2019 Feb.
44. Freitag N, et al. High-intensity interval training and hyperoxia during chemotherapy: A case report about the feasibility, safety and physical functioning in a colorectal cancer patient. Medicine (Baltimore). 2018 Jun; 97(24):e11068.
45. See https://en.wikipedia.org/wiki/Composition_of_the_human_body
46. Ippolito JE, et al. Extracellular pH Modulates Neuroendocrine Prostate Cancer Cell Metabolism and Susceptibility to the Mitochondrial Inhibitor Niclosamide. PLoS One. 2016; 11(7): e0159675.
47. Morgan D, et al. Voltage-gated proton channels maintain pH in human neutrophils during phagocytosis. Proc Natl Acad Sci USA. 2009;106:18022–18027.
48. Chao M, et al. A nonrandomized cohort and a randomized study of local control of large hepatocarcinoma by targeting intratumoral lactic acidosis. eLife. 2016; 5: e15691.
Sangeeta Pati, MD, FACOG, is medical director at SaJune Institute for Restorative and Regenerative Medicine (Orlando, Florida) since 2004. She specializes in bio-identical hormone therapy’s impact in regenerative medicine. She trains doctors in Regenerative Protocols That Work™ through the five-point model system. Her lectures have long been featured at A4M and AMMG. She may be reached through www.sajune.com.
John Apsley, MD(E), ND, DC, is an accomplished author and educational specialist. He teaches the general public how to properly set up their own regenerative lifestyles and offers medical consulting services exclusively to licensed healthcare providers. His lectures on regenerative medicine have been featured at A4M, Health Freedom Expo, the Trinity Conference, and as far away as Paris and China. He may be reached at john@drapsley.com.



