|
Originally published in Allergy Research Group Focus
Page 1, 2
This interview offers an introduction to Dr. Philip Miller's natural anticoagulant regimen. For a more detailed and comprehensive four-part tutorial on this subject of prevention of heart attacks and strokes (with numerous visually enhanced diagrams), please visit his website at www.antiaging.com, with accompanying blog posts at blog.antiaging.com.
 |
 |
Focus: On the website for your clinic, you offer a four-part, very detailed and fascinating description of a regimen you have developed to help prevent heart disease and stroke. What inspired you to craft this regimen?
Miller: About 1.5 million heart attacks and strokes occur every year in the United States, and one in every three deaths is due to cardiovascular disease.1 Cardiovascular disease is the number one cause of death globally.2 Everybody worries about a heart attack or stroke, especially if they're over sixty. People  worry that they're at risk. I developed this comprehensive approach over many years, and it is empirically derived, based on a good, fundamental knowledge of all the pathways in the body that contribute to acatastrophic vascular event. My approach relies on a novel combination of anti-fibrin and anti-platelet modalities. It is a rational approach that addressesthe entire coagulation cascade, from beginning to end. This includes platelet aggregation, fibrin deposition, markers of inflammation, and even the properties of red blood cells and why and how they stick together. worry that they're at risk. I developed this comprehensive approach over many years, and it is empirically derived, based on a good, fundamental knowledge of all the pathways in the body that contribute to acatastrophic vascular event. My approach relies on a novel combination of anti-fibrin and anti-platelet modalities. It is a rational approach that addressesthe entire coagulation cascade, from beginning to end. This includes platelet aggregation, fibrin deposition, markers of inflammation, and even the properties of red blood cells and why and how they stick together.
Fibrin Synthesis Cascade .pdf
My one emphatic caveat is that this regimen must be carried out under the care of a skilled and knowledgeable physician. You cannot self-treat, and nobody should abruptly stop a conventional anticoagulant routine. And let me emphasize, this proprietary anti-coagulation routine is prescribed only after starting our core program of select micro- nutrients and nutritional advice. We use CoQ10, taurine, d-ribose, and carnitine in high doses to support heart and brain function. It's all part of an integrative approach.
During the twenty years I've offered this regimen, I can't remember more than eight to ten patients who have suffered a major stroke or heart attack. This is out of thousands of patients, many of them older, with significant cardiovascular risk factors.
I monitor my patients regularly, and adjust the protocol when indicated. I also follow this approach myself, because I do not want to ever have a stroke.
Focus: What is your opinion of the conventional approach to coagulation?
Miller: It is certainly an interesting time in the treatment of stroke and heart attack. In the last few years, the FDA has a new class of oral anticoagulant drugs. Although their safety profile appears better than the old standby – coumadin (warfarin) – all three of the new medicines are blood thinners that can cause excessive bleeding and are to be used with caution in patients with kidney disease. Two of these new medicines lack an antidote in the event of a severe bleeding episode, which is of concern.3 An antidote has recently been approved for the third (dabigatran etexilate).4
Even with these advances in anticoagulant treatment, I still find the conventional, mainstream approach to stroke and heart attack to be too guideline driven. Some guidelines emphasize the prevention of platelet aggregation. Other guidelines emphasize the long-term use of anti-fibrin drugs. What is the best strategy? In this scenario, it depends on the guidelines. These evolving guidelines are determined by age, associated risk factors, and preceding conditions. The guidelines were originally developed to make decision-making simple, uniform, and coherent. But guidelines eventually become bloated and incoherent. They can read much like IRS tax code.5
Focus: Give us a quick précis of the conventional approach to preventing hypercoagulation.
Miller: The conventional approach to stroke and heart attack prevention starts by preventing platelets from clumping. Both aspirin and clopidogrel (Plavix) are drugs of choice. Aspirin is probably the safest conventional drug to help prevent heart attack and stroke. Clopidogrel is the second line of defense in antiplatelet therapy. It works by breaking down into metabolites, one of which binds irreversibly to a receptor on platelets. This prevents the platelets from aggregating and lasts the entire 7- to 10-day life of a platelet.
Then there are the standard anticoagulant drugs. Coumadin is the best known. Bleeding is the major adverse effect of warfarin. Hemorrhage may occur at virtually any site in the body.6,7 My biggest concern with warfarin is its mechanism of action. It depletes vitamin K reserves. There are seven vitamin K-dependent blood clotting ('coagulation') factors, and they are each important in the coagulation cascade that helps form a clot.8 Patients on warfarin are advised not to ingest any extra vitamin K and maintain a moderate, constant level of intake.9
Vitamin K is important for building bone.10-12 It helps regulate cellular growth, cell division, and both the developing and aging nervous system.13,14 Vitamin K is essential for matrix GLA protein activity, which prevents reverse calcium flow from bones into your arteries and heart valves.
Warfarin, by blocking vitamin K, can accelerate osteoporosis and arterial calcification.15-17 Healthy doses of vitamin K are vital to many functions. So, to me, the risk-benefit ratio seems questionable, especially if there are other, safer options.
Finally, there is a new class of anticoagulant drugs, called factor Xa drugs, which target the thrombin cascade. Thrombin is an enzyme that helps clots form. One molecule of factor XZa can cleave over 1000 molecules of prothrombin to thrombin.18 By cleaving prothrombin, factor Xa drugs can slow conversion to thrombin and reduce clots.
These newer drugs do not need frequent monitoring. They do not block vitamin K. Excessive bleeding is still their big risk, and one downside to direct factor Xa inhibitors is that, in most cases, there are no antidotes to unintentional overdose and a bleed. Taking vitamin K is a simple antidote to warfarin.
In addition, because these drugs are so new, eventually discover other long-term consequences that are not apparent yet.
Focus: What causes a stroke or heart attack?
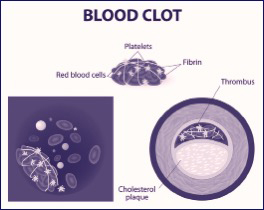
Miller: It all starts with the blood clot, which is essentially the eye of the hurricane. The blood clot is our body's universal mechanism for healing injury, and it usually results from injury. In the case of stroke or heart attack, it is an injury to the wall of a vein or artery. Take atherosclerosis, a condition where plaque builds up in the arteries over many years. Eventually, an area of plaque can rupture inside of an artery. The body attempts to repair that injury by forming a blood clot on the plaque's surface. If the clot becomes large enough, it can mostly or completely block blood flow, depriving tissues of oxygen (ischemia) and leading to stroke (cerebral infarction) or heart attack (myocardial infarction).
Atrial fibrillation, a heart arrhythmia, can also lead to a clot. In this case, the abnormal firing of electrical impulses causes the atria (the top chambers in the heart) to quiver. Blood flow slows down, and there is turbulence,19 which may lead to the formation of a clot. This type of arrhythmia is the most common type of irregular heartbeat and is found in 5% of those over the age of 65 and 10% of those over 80.20 Untreated atrial fibrillation increases the risk of a stroke by five-fold.21 Or alternatively, other research shows about 2% stroke incidence annually, in untreated atrial fibrillation.22
In both atherosclerosis and atrial fibrillation, the 'healing' clot may prove to be a problem.
Focus: So, the body's effort to heal an injury can sometimes backfire. What pathways and what cascade of reactions and interactions leads up to the clot?
Miller: Picture the blood vessel – a flexible tube through which your lifeblood is rushing at the astounding speed of three feet a minute the moment it leaves the heart.23 Every blood vessel is lined with endothelial cells, which form a protective lining called the endothelium. The endothelium secretes substances that stop those cascading blood cells from sticking to it.
 But when it is injured or damaged, the endothelium sends out distress signals. Those distress signals are picked up by platelets, tiny blood cells that help your body form clots. The platelets rush to the site of damage, ready to clump together (aggregate) and stick to the exposed wound and help form a clot. During and after aggregation, platelets continue to release substances that trigger further platelet accumulation and activation, as well as constrict veins and help form clots. Platelets are also involved in the inflammatory response and produce proinflammatory chemicals.24 But when it is injured or damaged, the endothelium sends out distress signals. Those distress signals are picked up by platelets, tiny blood cells that help your body form clots. The platelets rush to the site of damage, ready to clump together (aggregate) and stick to the exposed wound and help form a clot. During and after aggregation, platelets continue to release substances that trigger further platelet accumulation and activation, as well as constrict veins and help form clots. Platelets are also involved in the inflammatory response and produce proinflammatory chemicals.24
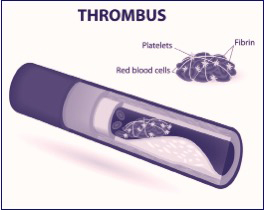
Platelets are significant in both atherosclerosis and in the development of stroke and heart attack. Aggregating platelets form the center of the growing clot.25,26 The clot in individuals who have died of a heart attack has a layered appearance, suggesting it has grown episodically over time.27
Once the initial platelet plug has formed, a second important pathway is initiated. This pathway involves the body's fibrin cascade. At first, thrombin is released. Thrombin is an enzyme in blood plasma that causes the clotting of blood. Thrombin converts fibrinogen, a soluble protein, to strong and insoluble fibrin molecules at the place of the wound. Shaped like long threads, the fibrin molecules interlace and crosslink with each other to form a kind of polymer mesh over the clot and stabilize it. It is a remarkable feat.
Under normal circumstances, your body has highly sensitive feedback systems to balance bleeding and clotting. Your body produces plasmin, an enzyme that degrades fibrin clots. And, to balance that dissolving process, you also produce inhibitors of plasmin.
So, to sum it up: injury or stasis, platelet plug, fibrin mesh, successful clot – but over time, potential infarction.
Focus: You've compiled a natural anticoagulation regimen that addresses all these pathways. Which natural molecules do you use and why?
Miller: I combine four simple but powerful constituents. They are nattokinase, Ginkgo biloba, high-dose fish oils, and vitamin E isomers. And, I emphasize adequate hydration – which means many glasses of pure water daily. Studies have shown that water can actually stop red blood cells from clumping as aggressively.
All of the above, when combined in proper doses by a physician, can be both gentle and potent. Every surgeon is now medically and legally required to ask, "What vitamins and herbs are you taking?" Every surgeon knowns that each and all of these agents I have discussed clearly have anticoagulant effects, but via different mechanisms.
Page 1, 2
|




