Online publication
only
Oxygen begot inflammation. Inflammation
begot the liver. The liver begot the
detox
pathways for endogenous
and exogenous poisons. Primordial
spherules forerunners
of modern cells formed, existed, and perished in the highly acidic and reducing
toxic soup. They consumed and thrived on the waste they created. Waste disposal
was not an ecologic issue then. All that changed when free oxygen in the
ambient air accumulated and brought forth a "reducing-to-oxidizing" shift
on the surface of the planet Earth. Then oxygen became the primary energy generator
of human biology by organizing the development of complex molecular pathways.
In those roles, oxygen also became the primary waste producer. Oxygen is the
ultimate Dr. Jekyll/Mr. Hyde, a spin doctor par excellence.1-4 Not
unexpectedly, it created dangerous oxyradicals as it differentiated, shaped,
and fine-tuned
the energetic chemistry of the human cells. Waste production created the
need for waste removal. Oxygen organized the designs for those systems as
well.
Sometimes oxygen clears waste by directly disintegrating it. We have white
beaches because oxygen oxidizes the black and brown organic matter washed
on them, turning it into carbon dioxide, water, and minerals. In other instances,
waste disposal requires a complex system for rapid disintegration of macro-molecules.
To that purpose, oxygen evolved the inflammatory response. The kaleidoscopic
mosaic of inflammation involves the following: (1) redox (oxidant/antioxidant)
regulation; (2) acid-alkali balance; (3) clotting-unclotting equilibrium;
(4)
sugar-based recognition systems; (5) lipid-based intelligence systems; (6)
protein-based systems of tissue construction; (7) enzyme-based systems of
deconstruction (including proteases and protease-inhibitors); and (8) scavenger
cells.1,5,6 Oxygen integrated the development, differentiation,
and maintenance of those systems most prominently in one body organ, the
liver. Highly specialized scavenger
cells in the liver are called the Kupffer cells. This, succinctly stated,
is my evolutionary perspective of oxygen, inflammation, and the liver.
The above evolutionary view integrates all known aspects of the epidemiologic,
experimental, biochemical, and clinical data concerning liver disease. Specifically,
it clarifies clinical thinking regarding the following: (1) the pathogenetic
mechanisms of liver diseases; (2) the roles of pathologic inflammatory responses
in ecologic, nutritional, and autoimmune disorders; (3) the response of the
liver to microbial infections in organs other than the liver; (4) objectivity
and quantifiabilty of the degrees of dysfunction of liver detox pathways;
and (5) scientifically sound liver detox and oxystatic strategies for reversing
disease. Later, I cite the findings of pertinent experimental studies to
further
shed light on the relationships between oxygen, inflammation, and the liver.
Below, I review aspects of anatomy, physiology, and pathology of the liver
to provide a framework of reference for presenting my clinical preferences
for liver detox.
The Liver Ecosystem
Nature is generous. Nature is stingy. Nature creates ample reserves. Nature
is a hard taskmaster. Nature is forgiving. Nature is unforgiving. Those are
all aspects of nature's grand plan of economy. In matters of human health,
next to the bowel, the liver is the most glorious mirror of nature's sense
of economy.
The liver weighs two-and-one-half to three pounds, yet it is the primary detox
and metabolic organ of the body. It not only nourishes 50-100 trillion cells
in the body, it is also responsible for keeping them clean and healthy. Thus,
it comes as no surprise that the liver is the most frequently stressed organ
of the body. One of the many wonders of nature is enormous functional reserve
of the liver. When 90% of the liver mass is removed in dog experiments, the
dogs stay healthy. In my biopsy work, I was more impressed by the regenerating
capacity of liver cells than that in any other organ.
The Eagle and the Liver
The ancient Greeks understood the liver's astounding ability to regenerate.
To punish the titan Prometheus for his transgression, the supergod Zeus had
him chained to a mountain and sent an eagle to lunch at the prisoner's liver.
Prometheus did not do too badly, however, as far as his liver was concerned.
The liver grew back every day by the time the eagle returned.
Mother Nature has designed the liver in a most extraordinarily loving way.
It has bestowed upon it a rare distinction: the liver gets its oxygen and nourishment
from two sources. One face of each liver cell fronts oxygen-rich blood from
the heart; the other is covered with nutrient-rich blood from the bowel. To
fully appreciate nature's benevolence, one needs to recognize that arterial
blood from the heart brings 40% to 50% of the required oxygen, while that from
the bowel delivers 50% to 60% of the liver's oxygen supply. That remarkable
fact explains why pathologists rarely see liver infarction (large areas of
cell death). The liver cell has yet another face that fronts ultramicroscopic
bile passages.
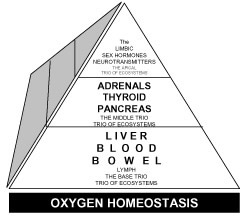
Why Is the Liver Included in the Base Trio of the Trios of Human Ecosystems?
Listed below are several metabolic, energetic, and detoxification distinctions
of the liver to support my inclusion of it in the base trio of The Pyramid
of Trios of the Human Ecosystem (Figure 1). In summary, the liver is all
of the following:
1. the master detox organ;
2. the master metabolic organ;
3. the master nutrition organ;
4. the master protein producer;
5. the master fat metabolizer;
6. the master sugar handler;
7. the master vitamin producer and processor organ;
8. the master mineral regulator organ;
9. the master hormone modulator;
10. the aging-gene organ; and, next to the bowel,
11. the master life span organ.
Figure 1. Schematic Representation of the Place of the Liver in the
Trio of Trios of Human Ecosystems for Preserving and/or Restoring
Oxygen Homeostasis
The
dual blood supply to the liver is a master stroke of nature's infatuation
with Dr. Jekyll/Mr. Hyde architectural designs. The blood from the bowel
not only brings nutrients and oxygen, but also a payload of natural and synthetic
toxins, chemicals, and toxic metals. It is the responsibility of the liver
to rid the entering blood of all toxic organic acids as well as other toxins
before the blood can spread the toxins throughout the body.
Liver Detoxification
It is one of the profound ironies of prevailing drug medicine that there is
no concept of liver detox among liver specialists. Treatment of most liver
diseases in the hands of gastroenterologists and hepatologists is confined
to the use of immune-suppressive therapies, such as steroids, chemotherapy
drugs, large doses of agents such as interferon, or liver transplants. Otherwise,
medical texts recommend "supportive treatment," which is a euphemism
for symptom suppression with drugs. In most patients with nutritional, ecologic,
immune, and heavy metal toxicity disorders, liver blood tests are often considered "within
normal limits," and no attempt is made to prescribe nutritional, herbal,
and natural detox therapies.
In contrast to gastroenterologists and internists, naturopaths nearly all develop
an abiding lifelong interest in this organ. That is so because the use of liver-friendly
nutrients, herbs, and liver detox is emphasized as the core strategy in their
schools. They recognize the clinical benefits of liver detox therapies, not
only in patients with known liver diseases but also with chronic immune, nutritional,
and ecologic disorders. Many of them are awkward in describing their concepts
of the structure and function of the liver. And yet, their clinical results
are superior to those obtained with drug therapies, except in cases of advanced
liver failure.
The Liver Has a Guardian Angel: the Bowel
The above statement is based on my work in surgery, pathology, and integrative
medicine over four decades. As a pathologist, I examined more than 14,000
bowel biopsies, 5,000 stomach biopsies, and 2,000 liver biopsies. In my clinical
work, I have cared for about 10,000 patients with chronic health disorders.
I realized some individuals recovered from chemical and microbiologic liver
injury expeditiously, while others developed long-lasting liver disorders.
I also recognized people in the latter group suffered from mold allergy,
adverse foods reactions, prolonged bowel transit time, increased bowel permeability,
and altered gut microbiota. Those observations led me to conclude a robust
alimentary tract guards the liver against indolent liver injury. Those observations
also led me to propose the schema of the Pyramid of Trios of the Human Ecosystem
(Figure 1).7,8
The study of urinary excretion of hippuric acid offers an unusual opportunity
to explore the relationships between the bowel and liver ecosystems for four
reasons: (1) it is produced in the liver by a conjugation detox reaction (of
benzoate with glycine) and so reflects the efficiency of this detox pathway;
(2) benzoate is produced in the gut by bacterial deamination of the amino acid
phenylalanine and so reflects the state of the bowel ecology; (3) benzoate
is present in many food preservatives and gives an indication of total chemical
load borne by the liver; and (4) pantothenic acid is the rate-limiting factor
in its production and so gives an estimate of the nutritional status of the
individual. For these reasons, I examined the relationships between increased
urinary excretion of hippuric acid and increased urinary excretion of seven
bowel-derived mycotoxins in 135 patients (Table 1). Note that increasing values
for urinary excretion of hippuric acid generally correlate with increased excretion
of mycotoxins, indicating impaired ability of the liver to effectively cope
with increased mycotoxin load produced by altered gut microbiota. It also furnishes
biochemical evidence of my view that the bowel serves as the guardian angel
of the liver.
From the Bowel to the Brain
The sick have a way of crystallizing the truth about illness. A fibromyalgia
patient once remarked, "Dr. Ali, for me, it's bowel to the brain. I
eat, and I get brain-fogged." I cannot think of a more succinct and
elegant way of stating the essential protective role of the liver. Medical
students are taught the same thing in many convoluted ways. (Perhaps that's
why they cannot seem to retain it when they leave medical schools.) In the
medical jargon, when the liver fails and toxins bypass it to reach the brain,
the problems of mood, memory, and mentation are designated as hepatic encephalopathy.
It is regrettable that so many physicians laugh at the concept of liver detoxification
and readily label the patients hypochondriacs when the cause of the patient's
suffer is liver toxicity. If the liver did not filter the blood of its toxins,
and the blood from the bowel were to hit the brain directly, everyone would
be brain-fogged at all times. I present this subject at length in Oxygen
and Aging (2000).9
Table 1. Relationship Between Increased Urinary Excretion of Hippuric
Acid and Increased Urinary Excretion of Bowel-Derived Mycotoxins*
| Hippuric Acid Excretion mol/mol creatinine |
Number of Bowel-Derived Mycotoxins Detected mol/mol
creatinine |
Group of Patients |
None |
1 |
2 |
3 and over |
Controls (n=66)**
Hippuric acid value below 400 |
13.6% |
25.8% |
30% |
30% |
Hippuric acid value 400-600
(n=24) |
12.5% |
29% |
29% |
32.5% |
Hippuric acid value 600-800
(n=12) |
8.3% |
41% |
17% |
33.3% |
Hippuric acid value >800
(n=33) |
6% |
24.3% |
21.3% |
48.3% |
*Mycotoxins profile included tartaric acid, arabinose, citramalic acid, three
furan compounds, and carboxycitric acid
**Normal hippuric acid excretion
I emphasize the bowel/liver dynamics here to underscore the importance
of undertaking robust measures to restore bowel ecology in all instances
of liver detoxification. I discuss this subject at length in Integrative
Nutritional Medicine, the fifth volume of The
Principles and Practice of Medicine.10
Castor-Cise: A Time for Healing
Once all indigenous cultures had healing rituals that provided people
with purpose and structure for physical and spiritual renewal. A
language of silence
was an integral part of most rituals. We now live "fast." What the
benefits are of the time saved is unclear to me. Those healing rituals have
fallen victim to the pace of modern life. Today we need healing rituals far
more than ever. In clinical medicine, I recognize the absolute need for regular
periods of physical and spiritual renewal that include the language of silence,
physical exercise, and detoxification measures.
We live in the age of toxic environment, toxic foods, and toxic thoughts. These
toxicities create a state of molecular and cellular burn-out. From the evolutionary
perspective of oxygen/inflammation/liver dynamics presented above, it should
be evident that the liver bears the brunt of such toxicities. For that reason,
I consider it essential to diligently assess the health of the liver in all
my patients with chronic and subacute disorders, and I recommend a robust liver
detox program to serve my overarching goal of restoring oxygen homeostasis.
Castor-Cise is my term for an integrated program that includes the following:
(1) a castor oil liver detox, based on the ancient Indian tradition; (2) a
castor oil bowel detox, based on the ancient Chinese tradition; (3) a sesame
oil oral detox, based on its empirical benefits; and (4) limbic, non-competitive,
meditative exercise. Below, I describe my own routine of Castor-Cise three
times a week. I regularly prescribe it for all my patients and strongly urge
them to be innovative once they have learned the basic routine. For most patients,
I also recommend the following: (1) a lemon juice-maple syrup "spicy lemonade" fluid
fast once weekly, which can be done on a scheduled Castor-Cise day; and (2)
Dr. Ali's breakfast five days a week (comprising two tablespoons of granular
lecithin taken with two tablespoons of freshly ground flaxseed and high-quality
protein powder mixed with 16 ounces of organic vegetable juice). See my column
in the May 2007 issue of the Townsend Letter11 and Integrative
Nutritional Medicine, the fifth volume of The
Principles and Practice of Medicine.10
Dr. Ali's Castor-Cise
On weekend mornings, I warm two tablespoons of castor oil in a large spoon
by flame. I apply the oil liberally to the following areas: (1) the liver
area (the rib cage on the right side, extending from mid-line in front to
the mid-line behind); (2) the front and sides of the abdomen; (3) shoulders;
and (4) face (a light smear). For the next two hours, I stay in a limbic
state, a meditative state free of the noise of a cluttered mind (see The
Cortical Monkey and Healing [1999] for detailed description).12 I do not
use the telephone or watch TV. Low volume music is acceptable at times. I
prepare my breakfast as described above (usually 60 ounces of my protein
shake) and take nutrient and herbal supplements with eight to ten ounces
of the shake at a time. Intermittently, I engage in limbic exercise (gentle,
non-competitive, meditative, described in my book The
Ghoraa and Limbic Exercise).13
I favor rebounding (jumping jacks on a rug wearing thick socks), rug-running,
and light weights (ten to fifteen pounds). There is no sweating, huffing,
or puffing, nor any sore muscles (crucial for a 67-year-old with much work
to do). In between segments of exercise, I practice limbic breathing (see
my column in July 2007 issue of the Townsend Letter14) and try to be in a
spiritual state (see my book The Crab, Oxygen, and
Cancer [2007]15 for practical
suggestions). I often work on my computer as well during Castor-Cise. Writing
comes easier in the limbic state. At the end, I shave, shower, and get ready
for the rest of my day. My shower begins with hot water and end with a sudden
burst of cold water. My sense is that the clinical benefits of the ancient
practice of sauna, followed by jumping in very cold water, accrue from improvement
of autonomic equilibrium. Each castor period is free of the demands of a
cluttered mind.
Castor-Walk, Castor Jog, Castor Gym, and Castor Sleep
There is a difference between teachers and gurus. True teachers want their
students to reach beyond their scope. Gurus do not want their disciples to
escape their servitude. In the spirit of teachers, I ask my patients first
to learn correctly Dr. Ali's Castor-Cise and then innovate and modify the
basic Castor-Cise routine to enhance its value for themselves personally.
For example, one can apply castor oil before going for a walk ("Castor-Walk"),
a jog ("Castor-Jog"), or a work-out in a gym ("Castor-Gym").
Many of my patients sleep with castor oil application ("Castor-Sleep").
Other patients do one, two, three, or all components of Castor-Cise, which
can be done on any given day, depending upon availability of time, mood,
or inclination. Again, the crucial point is that each castor period is free
of the demands of a cluttered mind.
The LEMP Spicy Lemonade Fluid Fast
Lemon juice, maple syrup, cayenne, and Epsom salt have been used for centuries
in various formulations for combined liver and bowel detox procedures. Below,
I describe the adaptation which my colleagues at the Institute of Integrative
Medicine, New York, and I have used for several years with empirical benefits.
The procedure is simple and, when done correctly (in a prayerful / meditative
state), does not cause any discomfort. The old "begin low-build slow
principle" is as applicable here as in other publications for medical
education. We do not find it necessary to alter the use of prescription medications
for our patients when they engage in the LEMP fast. We do reduce by 50% the
nutrient and herbal supplements during the first day of the fast.
I do not recommend a LEMP fast for periods longer than one day at a time, since
I have encountered adverse responses with extended fast/flushes. The amount
of needed Epsom salt varies with the condition of individuals. Two to three
quarts of additional water should be taken during the day. If hunger develops
and you become uncomfortable, a grapefruit may be eaten. A light vegetarian
meal is suggested for the evening if hypoglycemic symptoms occur. The following
is the two-part recommended protocol: Part A: Begin in the morning and continue
through the day with the spicy lemonade fluid consisting of: (1) two tablespoons
of fresh lemon juice; (2) two tablespoons of maple syrup (grade B); (3) one-half
teaspoon of cayenne powder (except in cases of gastritis and stomach ulcers);
(4) add 24 ounces of water, or more to the taste; and (5) drink in small portions
throughout the day, at your comfort level. May begin with a second 24-ounces
of the above. Part B: Begin the morning or mid-morning saline laxative with
one teaspoon of Epsom salt with three ounces of water. Slowly build to one
tablespoon, more if needed, for complete bowel evacuation.
Repeat after one hour (one tablespoon Epsom salt with three ounces of water),
if no bowel movement occurs. Repeat after one hour, if necessary. Hypoglycemic
symptoms develop uncommonly among our patients. Should symptoms occur, we recommend
drinking four ounces of a protein shake every four hours. If symptoms persist,
the LEMP fast should be terminated.
Liver-Friendly Nutrients and Herbs
Lecithin is the guardian angel of the liver. I prescribe it five days a week
for all my patients. Flaxseed and organic vegetable juice are my next priorities.
All three are included in Dr. Ali's breakfast. I prescribe liberal daily
doses of oxystatic nutrients, including glutathione (100-300 mg); co-enzyme
Q10 (100 to 200 mg); methylsulfonylmethane (MSM, 750 to 1,500 mg); taurine
(750 to 1,500 mg); and antioxidant vitamins. Among the minerals in elemental
doses are magnesium (500 to 750 mg); potassium (100 to 150 mg); calcium (500
to 750 mg); zinc (25 to 50 mg); and selenium, chromium, and molybdenum (400
to 600 mcg each). For oxystatic phytofactor support of the liver, I use the
following two combinations in weekly rotation: (1) milk thistle, 100 mg;
goldenseal, 50 mg; dandelion root, 50 mg; black radish, 50 mg; catnip, 50
mg; methionine, 400 mg; choline bitrate, 200 mg; and inositol, 20 mg; and
(2) red clover, 100 mg; tumeric, 100 mg; ginger, 100 mg; fennel seeds, 100
mg; Jerusalem artichoke, 100 mg; and tumeric, 100 mg. Onions, boswellia,
green tea, and rosemary are other suitable choices. In my view, it is crucial
to use herbs and phytofactors in rotation.
Direct Oxystatic Therapies
For reversing liver disease, my colleagues at the Institute of Integrative
Medicine, New York, and I rely heavily on direct oxystatic therapies, such
as hydrogen peroxide foot soaks, intravenous peroxide and ozone therapies,
and EDTA chelation infusions. I devote extended chapters to these therapies
in Darwin, Dysoxygenosis, and Oxystatic Therapies (2005)16 and Darwin,
Dysoxygenosis, and Disease, 3rd. Edition (2007),17 the third and eleventh volumes of The
Principles and Practice of Integrative Medicine.
Case
Studies
To illustrate the clinical benefits of oxygen-based
integrative management programs for liver detoxification and restoration
of liver health, in this
section, I present the following three case studies.
Case # 1: Reduction of Hepatitis C Viral Load
A 69-year-old man presented with a history of hepatitis C infection,
severe fatigue of three-years duration, hypertension, enlarged
prostate, nasal allergy,
constipation, impotence, and low blood immune cell count. His legs showed
dependent edema. With our integrative protocols and 14 intravenous hydrogen
peroxide infusions on a weekly or alternate-week basis, he showed slow
and steady improvement in symptoms of allergy, fatigue, and constipation
over
a period of twelve months. Table 2 shows how his hepatitis C viral count
dropped from over 5 million per ml to 489,230 per ml in about seven months
of oxy and antioxidant therapies. During that time, his immune cell count
rose from 2,900 to 3,600. Two months later, he developed upper abdominal
pain and was given antibiotic therapy for H. pylori for three weeks by
his gastroenterologist. When I saw him two months later, his viral
count had
climbed back to 1,879,000/ml, and his immune cell count had fallen to 3,000.
Table 2. Hepatitis C Viral Counts During Integrative Oxy Therapies
| Date |
Viral Count* |
WBC** |
Comments |
| 11/30/1998 |
over 5 million/ml |
2,900 |
Treatment begun |
3/13/1999 |
898,000/ml |
3,100 |
14 IV hydrogen peroxide on alternate weeks |
| 7/22/1999 |
489,230/ml |
3,600 |
Antibiotics received in September for an abdominal infection |
| 11/15/1999 |
1,879,000/ml |
3,000 |
Relapse of fatigue |
*Viral counts performed with RNA PCR technology and expressed as copies
per milliliter.
** White blood cells. Note how changes in the total viral count were
associated with the changes in the immune (white blood corpuscles)
cell count.
Case # 2: Increase in Hepatitis C Viral Load With Air Travel Dysoxygenosis
In Oxygen and Aging (2000),9 I introduced the term air travel dysoxygenosis
for a pattern of exacerbation of chronic disorders in the days and weeks
after extended air travel. In Table 3, I reproduce data from that volume
showing the values for hepatitis C viral during a four-year study period.
The patient responded well to our integrative therapies with focus on liver
detox and oxystatic therapies. A trip to Europe caused fatigue and abdominal
symptoms along with a dangerous rise in his viral load. Aggressive oxy therapies
dramatically lowered the viral count and restored his health within months.
Table 3. Changes in Hepatitis C Load With Air Travel Dysox
Dates
10. 06. 96
03. 22. 97
06. 17. 97
10. 07. 97
02. 06. 98
06. 19. 98
08. 06. 98
08. 27. 98
10. 28. 98
03. 08. 00 |
Hepatitis C Counts
203,000
1,078,000
1,731,000
414,000
367000
2,133,000*
926,000
497,000
118,308
199,000 |
*He traveled to Europe and developed abdominal discomfort and fatigue within
a few days of the trip. He felt better while traveling in Europe by car. After
the return flight, he became ill.
Case # 3: Recovery from Chronic Hepatitis Associated with Crohn's
Colitis
In 1993, a 51-year-old attorney presented with chronic fatigue, myalgia, inhalant
allergy, and intractable diarrhea. He had undergone colectomy for Crohn's colitis.
Liver function tests revealed evidence of severe hepatic inflammation caused
by ascending cholangitis secondary to chronic inflammation of rectum. He responded
well to our liver detox and oxystatic therapies. His liver function tests showed
of marked reduction in liver inflammation. Three years later, he was unable
to follow the program and suffered a severe attack of proctitis, which caused
a relapse of hepatitis. Table 4 shows the data concerning his liver function
tests performed over a period of fourteen years.
Table 4. Normalization of Abnormal
Liver Enzyme Levels*
| |
GGTP |
ALT |
AST |
Alk Phos |
Globulin |
| Nov. 1993 |
1670 |
131 |
101 |
522 |
3.6 |
| June 1994 |
928 |
76 |
46 |
291 |
3.4 |
| Feb. 1996 |
158 |
76 |
44 |
158 |
2.9 |
| March 1996 |
814 |
39 |
49 |
N/A |
4.1 |
| Sep. 2006 |
145 |
26 |
40 |
117 |
3.5 |
| May 2007 |
487 |
47 |
34 |
140 |
3.4 |
* Laboratory reference ranges: GGTP, 0-65IU/L; ALT, 0-55 IU/L; AST, 0-40 IU/L;
Alk. Phosphatase, 20-160 IU/L; Globulin, 1.5 to 4.5 g/dL.
Oxygen, Liver Injury, and Regeneration
The German chemist De Groot and colleagues investigated lipid peroxidation
and cell viability in isolated liver cells.18 They designed an oxystat
system capable of maintaining steady-state oxygen partial pressures (PO2) in
incubating
and respiring cells at levels between 0.1 and 300 mm Hg for days. Not unexpectedly,
at PO2 between 35 and 70 mm Hg, carbon tetrachloride (CCl4) induced lipid peroxidation
and death in the liver cells. Interestingly, under anaerobic conditions and
at PO2 greater than 70 mm Hg, CCl4 did not destroy any liver cells. Evidently,
both the lack of oxygen and very high levels of oxygen stopped liver metabolism
and saved the cells from CCl4 toxicity.
In the second study, the Italian researcher Bruno Nardo and colleagues examined
the protective effects of additional oxygen supply on liver regeneration following
CCl4 toxicity and partial hepatectomy in rats.19 They performed portal vein
arterialization (PVA) by interposing a stent between the left renal artery
and splenic vein after left nephrectomy and splenectomy. They observed a rapid
regeneration leading to the resolution of toxic-induced massive liver necrosis
and a faster restoration of liver mass after partial hepatectomy.
In the third study, the Japanese investigator Kabuto and colleagues investigated
the changes in antioxidant systems of the liver cells caused by bisphenol A
toxicity.20 They observed the following: (1) increased levels of reduced glutathione
(GSH) and glutathione disulfide (GSSG); (2) increased superoxide dismutase
(SOD) and decreased catalase activities; and (3) increased activity of glutathione
peroxidase (Gpx) activity, which is expected to readily convert hydrogen peroxide
to hydroxy radical.
In the fourth study, the Japanese investigator Tomarui and colleagues examined
the effects of diesel exhaust particles (DEP) on the liver cells.21 Pulmonary
exposure to DEP caused fatty change of the liver in obese diabetic mice via
oxidative stress. I cite this study to underscore the importance of including
pollutants in the ambient air among the causes of liver injury. Earlier, I
indicated that I examined over 2,000 biopsies in my hospital pathology work.
I do not recall a single time when any gastroenterologist or hepatologist ever
brought up this subject while reviewing a liver biopsy with me.
Concluding Comments
Evolution of oxygen-driven, high-efficiency cellular energetics was one of
nature's master strokes. Oxygen, the ultimate, elemental Dr. Jekyll/Mr. Hyde,
generates both clean energy and toxic waste. The design of the inflammatory
response under the organizing influence of oxygen was nature's other trump
card. The inflammatory response, a requisite for cellular healing, is a kaleidoscopic
mosaic. In a previous article, I drew a sharp distinction between physiological
and pathological inflammatory response.4 Next to the bowel, the liver protects
the integrity of that mosaic more than any other organ. In this article,
I develop a new line of biochemical evidence to support that view by presenting
a large body of personal data that correlate increased urinary excretion
of hippuric acid with increased urinary excretion of bowel-derived mycotoxins.
Castor-Cise is my integrated program of a castor oil liver detox, a castor
oil bowel detox, a sesame oil oral detox, and limbic, non-competitive, meditative
exercise. I hope readers will consider my regimen and put it to a clinical
test of validation. Finally, I have presented case histories to illustrate
the potential benefits of integrated liver detox program.

Notes
1. Ali M. Spontaneity of Oxidation in Nature and
Aging (monograph). Teaneck,
New Jersey: 1983.
2. Ali M. The Principles and Practice of Integrative
Medicine Volume I: Nature's Preoccupation With Complementarity and Contrariety.
New York: Canary 21 Press. 1998. 2nd edition 2005.
3. Ali M. September Eleven, 2005. New York: Aging
Healthfully Book; 2003.
4. Ali M. Oxygen governs the inflammatory response and adjudicates the man-microbe
conflicts. Townsend Letter. 2005;262:98-103.
5. Ali M. The dysox model of aging. Townsend Letter. 2005;269:130-134.
6. Ali M. Darwin, oxidosis, dysoxygenosis, and integration. J
Integrative Medicine.
1999;3:11-16.
7. Ali M. The Principles and Practice of Integrative
Medicine Volume V: Integrative Immunology. 2nd edition. New York:
Canary 21 Press; 1999.
8. Ali M. Recent advances in integrative allergy care. Current
Opinion in Otolaryngology & Head
and Neck Surgery. 2000;8:260-266.
9. Ali M. Oxygen and Aging. 2000. New York:
Canary 21 Press; 2000. New York: Aging Healthfully Books; 2000.
10. Ali M. The Principles and Practice of Integrative
Medicine Volume V: Integrative Nutritional Medicine. 2nd Edition. New York: Canary 21 Press;
2001.
11. Ali M. The dysox model of diabetes and de-diabetization potential. Townsend
Letter. 2007; 286:137-145.
12. Ali M. The Cortical Monkey and Healing. Bloomfield, New Jersey: Life Span
Books; 1991.
13. Ali M. The Ghoraa and Limbic Exercise. Denville, New Jersey: Life Span
Books; 1993.
14. Ali M. Limbic breathing. Townsend Letter. 2007; 288:160-166.
15. Ali M. The Crab, Oxygen and Cancer. Volume I:
The Dysox Model of Cancer.New
York: Canary 21 Press; 2007.
16. Ali M. The Principles and Practice of Integrative
Medicine Volume III: Darwin, Dysoxygenosis, and Oxystatic Therapies.
2nd Edition. New York: Canary 21 Press; 2005.
17. Ali M. The Principles and Practice of Integrative
Medicine Volume XI: Darwin, Dysoxygenosis, and Disease. 3rd edition.
New York: Canary 21 Press; 2007.
18. De Groot H, Littauer A, Hugo-Wissemann D, et al. Lipid peroxidation and
cell viability in isolated hepatocytes in a redesigned oxystat system: evaluation
of the hypothesis that lipid peroxidation, preferentially induced at low
oxygen partial pressures, is decisive for CCl4 liver cell injury. Arch
Biochem Biophys. 1988;264:591-9.
19. Nardo B, Caraceni P, Puviani L, et al. Successful treatment of CCl4-induced
acute liver failure with portal vein arterialization in the rat. Journal
of Surgical Research. 2006;135:394-401.
20. Kabuto H, Hasuike S, Minagawa N, et al. Effects of bisphenol A on the
metabolisms of active oxygen species in mouse tissues. Environ
Res. 2003;93:31-5.
21. Tomarui M, Takano H, Ken-Ichiro Inoue, K-I, et al. Pulmonary exposure
to diesel exhaust particles enhances fatty change of the liver in obese diabetic
mice Int. J. Molecular Medicine.
2007;19:17-22.
|



