By Scott C. Cuthbert, DC
Introduction

Early in the development of applied kinesiology, Goodheart (1965) observed a fairly consistent relationship between weak muscles associated with specific organ or gland dysfunction. Goodheart noticed that when an organ or gland was in a state of dysfunction, there was usually a specific muscle or group of muscles that would be inhibited when assessed by manual muscle testing.
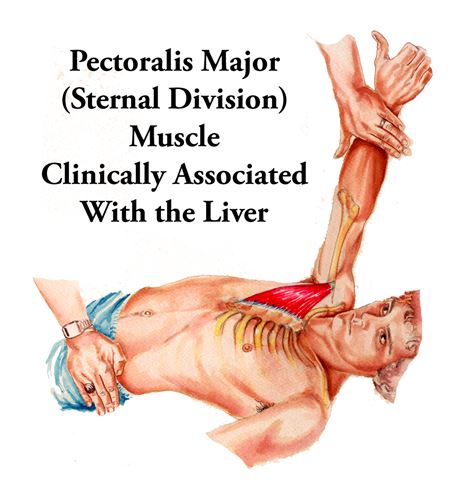
The first therapeutic approach that recognized this association—other than simply correlating a pectoralis major (sternal division) weakness with liver problems—was Chapman’s lymphatic reflexes. Chapman, an osteopath, used these reflexes to enhance lymphatic drainage of organs and glands. The Chapman reflex, which influenced the sternal division of the pectoralis major muscle, was the liver reflex. In applied kinesiology, Chapman’s reflexes are referred to as neurolymphatic reflexes. These were correlated with muscular weakness by Goodheart for muscle-organ/gland associations throughout the body.1
Applied kinesiology (AK) evaluates muscle function using the manual muscle test (MMT), a diagnostic test that has shown good reliability and validity for patients with muscle strength impairments.2-3 The use of MMT procedures is for three purposes in AK: (1) to aid in the diagnoses of structural, chemical, and/or mental aspects of health dysfunctions, (2) to offer the potential for shortening the course of treatments through “challenge” procedures, and (3) to determine the effectiveness of treatments. In so doing, AK’s testing methods used for the discovery of structural, chemical, or biopsychosocial disorders that produce these muscle strength impairments guide the treatment given to the patient.2-5, 10-11
In AK, muscular dysfunction is thought to reflect neural function. First the Kendalls in the 1950s,2, 12then Goodheart and Janda in the 1960-1990s,13 followed by many others have expanded the construct validity and the clinical usefulness of the MMT2-21because of the recognition that muscular imbalance is a key characteristic of spinal, neuromuscular, and articular dysfunction. AK suggests that muscle function is a transcript of the central integrative state of the anterior horn motoneurons, summing all excitatory and inhibitory inputs.11 In other words, the locus of muscular dysfunction ultimately rests with the nervous system.
AK is a diagnostic and therapeutic technique that has gained peer-reviewed published support within the chiropractic, medical, osteopathic, dental, biofeedback, acupuncture, veterinary, and other health care literature.15-20The research underlying the AK manual muscle testing procedures as this relates to the treatment of female and male endocrinopathies has some substantiation as well.2, 18-21, 24
Clinical Features
A twenty-year-old female presented to our Makati, Manila Philippines, office for help with severe premenstrual abdominal pain and irregularity since the start of her menstrual periods. Her gynecologist treated her problem medically in 2018 with the insertion of a hormonal IUD (intrauterine device). This procedure exacerbated her chronic menstrual problems. Because the IUD would not be removed during the course of her treatment, the clinical thought process involved assessing the patient for excess progesterone and estrogen, which are the hormonal components of the IUD.
Energetic testing of separate vials of estrone, B-estradiol, as well as progesterone, weakened the patient’s previously strong indicator muscles. However, with simultaneous (or “two-point”) therapy localization (TL)26 to the alarm point for the liver, this muscle inhibition was negated, indicating that the liver was failing in its role of detoxifier for the body and that she had abnormal amounts of estrone, B-estradiol, and progesterone hormones in her system.

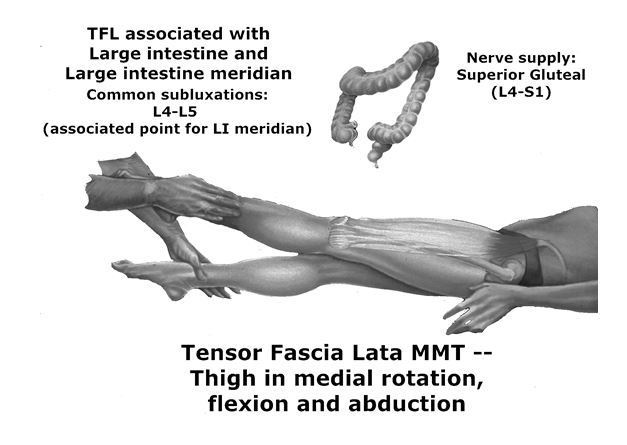
Additionally, positive therapy localization to the large intestine’s viscerosomatic reflexes was positive, and simultaneous (or “two-point”) TL to the liver cleared this problem as well, the patient was advised to go on a broad-spectrum antimicrobial, (anti-fungal, anti-bacterial, anti-viral, anti-parasites), anti-inflammatory, and immune stimulant herb to reduce the burdens on the liver. Morinda citrifolia (also known as noni) has been used for hundreds of years throughout Polynesia for a variety of conditions.25 Morinda has been shown to increase dopamine and serotonin, which could help alleviate depression. It has been used as a folk remedy for depression for hundreds of years, and this is a potential explanation behind why it has traditionally helped. This patient has been so pleased with the use of Morinda that she now says, despite her restoration to an asymptomatic state, that “I am afraid to go without it.”
The first treatment consisted of the detection of numerous viscerosomatic reflexes related to her endocrine system, primarily the liver, bowels and adrenal glands. The viscerosomatic reflex arises from afferent stimuli coming from visceral disturbances. These modify somatic tissues, particularly the skeletal muscles and skin overlying the dorsal horn of the spinal cord near the segmental level that supplies the organ involved.2Palpable tenderness and decreased and increased skeletal muscle tone have been shown to result from nociceptive viscerosomatic stimuli.
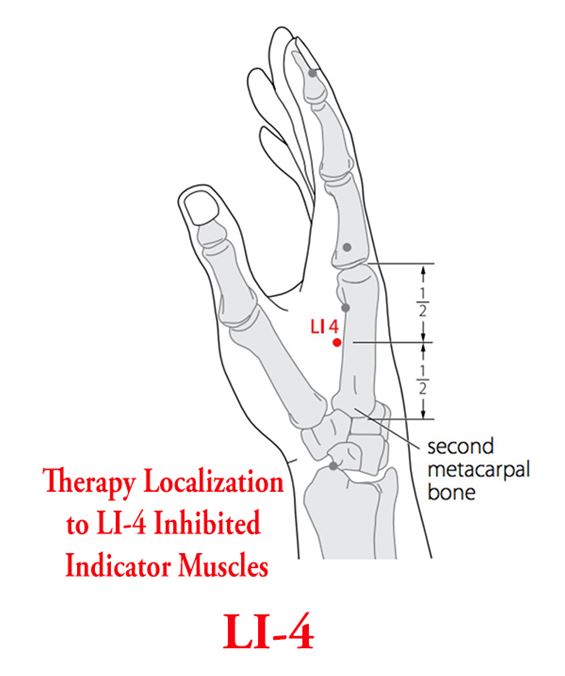
The pectoralis major (sternal division) muscle is associated with the liver.2 It has been clinically realized that liver dysfunction permits excessive hormones to produce symptoms in the patient, as the job of the liver is to both filter the hormones and the bowel. Bowel dysfunctions were also related in the patient’s history; and therapy localization to the alarm point of the bowel and the acupuncture point LI-4 (large intestine 4, the so-called “Source point” for the large intestine meridian in Traditional Chinese Medicine) were present.
The clinical deduction was made that relieving the liver of the distress it was undergoing from the patient’s bowel dysfunction, would improve the liver’s capacity to better filter the excess hormones coming from her IUD, producing her menstrual problems.
From a biochemical point of view, just before menstruation the liver must conjugate (prepare for elimination) increased amounts of progesterone and rising amounts of estrogen. By leveraging a woman’s web of endocrine wellness to do this, the body’s excretion of these hormones on a monthly basis occurs smoothly with very little, if any, symptomatology. The primary job of the liver is “to clean the bowel.” Whenever a patient has a hormone imbalance, a bowel disruption, or a liver problem, the other interacting aspects of their glandular and digestive function must be addressed for complete restoration of health. With this therapeutic approach, PMS can become a thing of the past.
On her first visit, inhibition of the sternocleidomastoid muscle was also corrected with treatment of the cranial system, involving inspiration and expiration assist cranial dysfunction corrections. This scenario has been reported dozens of times in the Collected Papers of the International College of Applied Kinesiology by physicians practicing AK around the world.1-2, 21 In fact, up-regulation of the signal from the neuro-endocrine axis to the ovaries (from the reduction of the cranial system dysfunctions) can create the onset of a menstrual period within minutes. It is our observation that cranial stress resolution through chiropractic manipulations to the skull and TMJ upregulates both the pineal and pituitary glands, allowing them to fully function as the master neuroendocrine transducers amplifying the innate intelligence of the neuroendocrine system and improving the HPA-axis.
Gastrointestinal irritation and/or inflammation may be caused by dietary imbalances, allergy, stress factors, local bowel flora changes due to use of medication (e.g., antibiotics), environmental pollution or other factors, resulting in altered gut ecology. This process involves depleted beneficial bacterial function, reduced protective secretory IgA levels and increased gut permeability.
This sequence of adaptations to previous or ongoing events results in larger than desirable molecules being absorbed from the gut, potentially triggering allergic reactions, as well as overloading liver function, with the possibility of autoimmune and hormonal consequences. The patient’s excessive pain syndromes and hormonal imbalances were likely related to this pattern of inflammation from the gut mucosa.
Results
The correction of cranial and spinal dysfunction, in addition to the use of Morinda for the bowel, as well as milk thistle for the liver, and ashwagandha for the adrenal glands brought about a rapid improvement in this patient’s clinical picture. The clinical findings of the first four visits are reviewed in Table 1, below.
| AK examination finding | Corrective Treatment/Outcome |
| Sternocleidomastoid (SCM) on the left and anterior scalene muscles inhibited bilaterally | Right inspiration, left expiration assist cranial fault corrections to the temporal bones bilaterally (strengthened SCM on left and anterior scalene bilaterally) |
| Positive therapy localization (TL) and challenge (producing inhibition to previously strong indicator muscles) to the left TMJ on sagittal opening of the jaw | Strain-counterstrain and percussion used on the medial and lateral pterygoid muscles (this muscle surrounds the eustachian tube) and abolished challenge and TL to the left jaw on sagittal opening |
| Positive challenge (producing inhibition to previously strong indicator muscles) for a category I pelvis with a right posterior ilium | SMT (spinal manipulative therapy) to the pelvis (DeJarnette wedges) abolished challenge to the pelvis and strengthened the left hamstring muscle |
| Positive TL to acupuncture point Large Intestine 4 (LI-4) and the alarm point for the Large Intestine (ST-25) (TL to LI-4 and ST-25 produced inhibition in previous strong indicator muscles). | Simultaneous TL to the alarm point for the liver corrected challenges to the bowel viscerosomatic reflexes |
| Positive TL to neurolymphatic reflex (NL) for the adrenal glands and emotional neurovascular reflexes (produced inhibition in previous strong indicator muscles) | Use of Ashwagandha corrected both findings |
| Bilaterally inhibited gluteus maximus muscles | SMT for upper cervical fixations strengthened gluteus maximus muscles bilaterally |
One week later the patient was seen for her second visit. She was moving her bowels twice a day and no longer had any low back pain. We found and corrected a category one right, pelvic-spinal subluxation, TMJ muscle imbalances, and bilateral talus bone joint dysfunctions in the feet.
The patient was seen a week later, and she noted that her period had passed with very little pain, right on time, and of the correct length, for the first time in over two years. She continued to feel better and was happy with the outcome. Her anxiety levels were markedly reduced after the initial correction of a hyperventilation syndrome or breathing pattern disorder, found with muscle testing to be a failure of all indicator muscles on full expiration challenge. Her sleep was also improved with the reduction in her anxiety.22 We found and corrected a category 1 pelvic-spinal subluxation, with C4 PR. The patient reports that she has also lost weight and inches around her waist and has found this pleasing and noteworthy.



