Editor’s Note: Exposure to mold in water-damaged buildings causes a frustrating number of puzzling symptoms and eventually leads to chronic inflammatory response syndrome (CIRS), as explained in the first article of this five-part series, published in the July 2019 issue. In Part 2 (August/September 2019), the authors explained the importance of maintaining the building envelope in order to prevent health-damaging mold from infesting buildings.
By Ritchie C. Shoemaker, MD, Medical Director, Center for Research on Biotoxin Associated Illnesses;
David Lark, Mycologist, MouldLabs, Australia;
James C. Ryan, PhD, Chief Science Officer, ProgeneDx
CIRS Diagnosis

When we think of chronic inflammatory response syndrome (CIRS) in 2019, our initial case definition has been expanded to include not only
1. abnormal proteomics;
2. abnormal regulation of immune functions and hormonal feedback loops;
3. loss of neuropeptide regulation of the above;
4. but also, abnormal transcriptomics;
5. together with suppression of ribosomal and nuclear encoded mitochondrial genes.
In the text that follows these terms will hopefully become clear and begin to act as your friend. Suffice to say, these CIRS illnesses are all around you; but of possible greater importance, the concepts of 6. dysregulation of inflammation and 7. dysregulation of gene transcription set the precedent for looking at underlying inflammatory bases for other illnesses, including autoimmune problems, diabetes, obesity, atherosclerosis, and neurodegenerative processes in a new light.

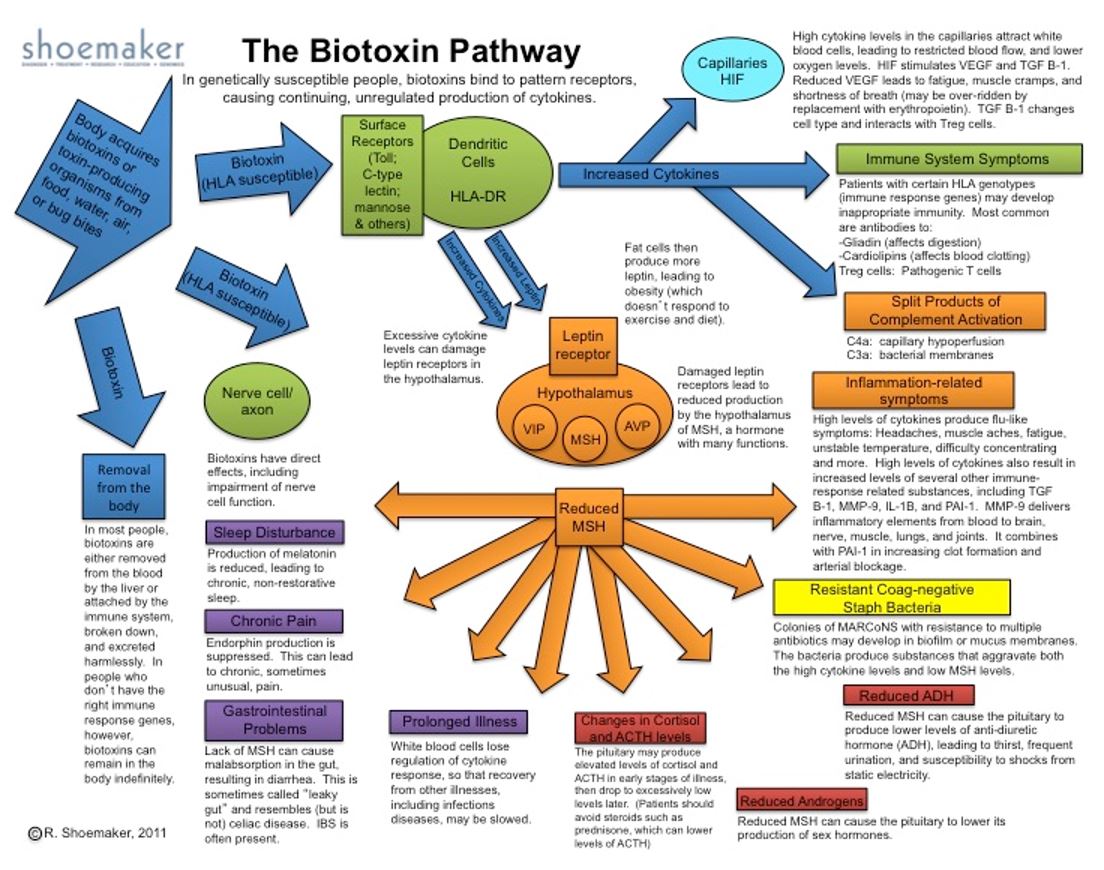
Clinical Case Definition: Chronic inflammatory response syndrome (CIRS) is a chronic illness acquired following the exposure to the interior environment of a water-damaged building (WDB) with resident microbes including, but not limited to, filamentous fungi, bacteria, including actinomycetes and mycobacteria; and their toxins and inflammagens, including, but not limited to, hemolysins, beta glucans, mannans, and spirocyclic drimanes. Cases with CIRS-WDB will have multisystem, multi-symptom illness. Presence of multiple reliable objective biomarkers, taken as a group but not individually, will aid in diagnosis and in monitoring therapy. Markers include genetic haplotypes, innate immune inflammatory elements, deficiency in neuroregulatory peptides or their receptors, dysregulation of pituitary and end organ endocrine factors, as well as clearly defined abnormalities in transcriptomics.
Perhaps of the greatest diagnostic and therapeutic importance is the finding of a marked suppression of 1) ribosomal; and 2) nuclear encoded mitochondrial genes in CIRS patients before treatment.
There are at least 30 entities found inside WDB that individually and collectively can set off innate immune responses.1 Indoor exposure will perpetuate these responses with eventual differential gene activation providing a mechanism for inflammatory compound production in the absence of ongoing exposure. Some of these inflammatory elements are well known. Endotoxins made by Gram-negative rod bacteria and actinomycetes, long overlooked but of marked importance and second only to endotoxins as activators of dysregulated gene activity, all cause differential gene activation.
We also know there is a pathogenic role for mycotoxins, albeit much smaller than thought just a few years ago. As additional research is becoming clear, mycolactones, made by mycobacteria, also have an inflammatory role. Of importance, are beta glucans, mannans, hemolysins, proteinases as well as cell wall fragments, hyphal fragments, and particulates found in reservoirs in air, including small, fine and ultra-fine particulates. We have not yet defined adequately a pathogenic role for mVOCs (microbial volatile organic compounds), but consensus opinion supports mVOCs having some ill-defined role in creating adverse human health effects. References for these important entities are found in the 2015 Medical Consensus Report on the Surviving Mold website.

Differential Diagnosis, Other CIRS: Even though CIRS caused by exposure to the interior environment of WDB remains the most important source of CIRS, there are other important exposures that must be included in differential diagnosis. These include consumption of ciguatoxic fish found on tropical reefs. We must also look to see if there is exposure to freshwater bodies with resident blue green algae (cyanobacteria), found in every state of the Union. CIRS is also found in post-Lyme syndrome2 and the rarely observed bites from recluse spiders. Of interest, is the discussion coming from the chronic fatigue syndrome (CFS) community commenting on CFS as a CIRS as well. Traumatic brain injury, including concussion and repetitive head injury from either concussive force such as firing artillery weapons or athletic competition with head contact, can set off innate immune responses that appear similar to CIRS is some ways.
Federal Agency Case Definition: In 2008, the US GAO provided us with a federal agency approved case definition that includes (1) potential for exposure; (2) symptoms like those seen in published, peer-reviewed literature; (3) laboratory findings similar to those seen in published, peer-reviewed literature and (4) response of objective parameters to treatment. This case definition provides flexibility for the clinician but also demands a benchmark of documentation of objective parameters to be found before a person can be labeled as having CIRS or an illness caused by exposure to a wet building.
In differential diagnosis, a process that sorts illnesses from non-illnesses, we will see normal laboratory findings of ESR, CRP, CBC and CMP. In addition, CIRS usually has normal thyroid functions, ANA, total IgG, total IgE and IgM. Cholesterol will be normal, and serum protein electrophoresis is normal. Viral studies are often thought to be indicative of ongoing viral infection but according to transcriptomic data are just telling us about intercalation of viral DNA into our own DNA. CIRS cases will usually have a normal EKG, normal pulse oximetry, and normal chest x-ray. There are interstitial lung disease findings less commonly found in CIRS so that chest x-ray must be obtained and reviewed. Of possible interest is the finding that certain cancers are under-represented in CIRS compared to the normal population. These include colon cancer, adenocarcinoma of the lung, and breast cancer (unpublished clinic data).
Looking for biomarkers, VCS (visual contrast sensitivity) deficits are found in 92% of CIRS cases. Analysis of symptoms, using cluster analysis (see Table 1), shows unique findings of 8 of 13 clusters found in adults with CIRS. Children are less often found to have distinctive clusters but finding 6 of 13 is consistent with CIRS in pediatrics. As an aside, reliable peer-reviewed literature3 has shown that CIRS can extend to single symptoms in children with an emphasis of chronic headache and chronic abdominal pain.
Table 1. Cluster Analysis of Symptoms
Individual categories:
1. Fatigue
2. Weak, assimilation, aching, headache, light sensitivity
3. Memory, word finding
4. Concentration
5. Joint, AM stiffness, cramps
6. Unusual skin sensations, tingling
7. Shortness of breath, sinus congestion
8. Cough, thirst, confusion
9. Appetite swings, body temperature regulation, urinary frequency
10. Red eyes, blurred vision, sweats, mood swings, icepick pains
11. Abdominal pain, diarrhea, numbness
12. Tearing, disorientation, metallic taste
13. Static shocks, vertigo
A positive cluster analysis for biotoxin illness is presence of 8 or more of 13 clusters.
Finding a combination of VCS deficits and positive cluster analysis results in a 98.5% accuracy shown for CIRS with a 1.5% total source of abnormalities in false positives plus false negatives.
On physical exam, it is common to find a resting tremor in cases with this finding best observed by having the patient hold their hands out straight with palms facing down to the floor, spreading fingers as wide as possible. Then a single sheet of paper is placed on the outstretched hands; the fine tremor is easy to see. Hypermobility is commonly seen as well, particularly in those with antigliadin antibodies and anticardiolipin antibodies.
Additional laboratory findings include a distinctive HLA-basis of susceptibility with increased relative risk (RR >2.0); levels of MSH lower than 35 pg/ml; high levels of C4a, TGF beta-1 and MMP-9; with dysregulation of ACTH relationship to cortisol and antidiuretic hormone (ADH) relationship to osmolality. Commonly, there will be either low or high VEGF with one-third of cases each being under 31 or over 86. An abnormal von Willebrand’s profile will be found in approximately 66% of patients. Nasal culture showing multiple antibiotic-resistant coagulase negative staph (MARCoNS) will be found in the deep aerobic nasal space in over 80% of cases with low MSH. Of these MARCoNS, over 60% will be resistant to methicillin.
An aside about mycotoxicosis: Since the advent of the shotgun use of antifungal medications to treat “mycotoxin illness,” a re-run of what we saw in the ENT literature of the early 2000s, there has been an explosion of creation of frightening antibiotic resistances found in these MARCoNS, known promiscuous exchangers of plasmids and circular DNA, especially when antibiotics and antifungals are used together. Our antibiotic, biofilm-busting nasal sprays that worked wonders with “pre-2015 MARCoNS,” no longer worked when azoles were added to sprays. These resistances include resistance to vancomycin and gentamicin! There are multiple additional reasons to not use anti–fungals indiscriminately, as will be discussed.
Our concerns about unwarranted use of antifungals for mycotoxicosis go to more than the current explosion of deaths from multi-azole resistant Candida auris, called a “serious global health threat by the CDC” (CBS News 4/9/19); it goes to claims of illness using findings of mycotoxins in urine to diagnose the condition. Yet, there is no published control group data (PubMed search 4/9/2019) showing absence or simply a paucity of mycotoxins in urine in controls compared to cases. Moreover, when we look at the world’s literature on urinary mycotoxins, we find scores of papers regarding healthy people with markedly abnormal levels of mycotoxins in urine.
As one reviews findings in CIRS beyond symptoms, VCS, and laboratory findings, depressed VO2 max and reduction reduced anaerobic threshold stand out. These findings, with low VO2 max thought to be related to ME/CFS,4 are typically found in all sources of CIRS. Simply stated, if one is given capillary hypoperfusion, as seen in CIRS, reduced VO2 max will invariably be found. One must also review the section below on hypometabolism, as our thinking on VO2 max has been radically modified by new data coming from transcriptomics.
“Of all the things I have lost, I miss my brain the most.“
We also see elevated pulmonary artery pressure at rest (≥ 30 mm Hg) in CIRS but more often we can confirm that in exercise, PASP pressure usually rises more than 8 mm over baseline in CIRS patients.5 This problem is called acquired pulmonary artery hypertension.
“Of all the things I have lost, I miss my brain the most.” There is a uniquely abnormal fingerprint for CIRS-WDB found on NeuroQuant (NQ) with published evidence so strong that NeuroQuant is now one of the primary ancillary studies that should be done in all patients over age 7 and under age 92.6-8 We have come to conclude that NQ is uniquely able to demonstrate the dreaded complications of multinuclear grey matter atrophy.

Of significant concern is the increased incidence in CIRS of lateral ventricle enlargement suggesting normal pressure of hydrocephalus but also suggesting atrophy of cortical grey matter. This atrophy extends to grey matter nuclei, which will have a mean incidence of 2.4 out of 6 grey matter nuclei in CIRS-WDB. Post-Lyme syndrome patients show mean atrophy of 3.0/6.
For those patients who have been treated with antifungals, a total of 4.5/6 atrophic grey matter was confirmed.9 I don’t understand taking medications that are optional at a cost of structural brain integrity.
With an eye towards defective antigen presentation, we know that there is no protection from other sources of CIRS provided by a given source of CIRS. Our concepts of an active and effective adaptive immune response don’t necessarily apply to CIRS.
Transcriptomics: Perhaps of greatest diagnostic and therapeutic importance is the finding of a marked suppression of (1) ribosomal; and (2) nuclear encoded mitochondrial genes in CIRS patients before treatment. Recovery with use of a published, peer-reviewed protocol (the Shoemaker protocol) has brought new hope that we will finally be able to put aside the longstanding dogma that these illnesses are never cured.
Because of the common findings of CIRS, with over 50% of buildings in the US reportedly having water intrusion and microbial growth, it is a tautology that CIRS doesn’t hide.
Unfortunately, CIRS is uncommonly diagnosed outside of the communities dedicated to CIRS. It is quite rare, however, to find patients or providers who don’t know someone who is chronically ill from fibromyalgia or CFS. Those diagnoses are ones without objective diagnostic biomarkers; not to mention none that also guide therapy. Once physicians can fill in the CIRS gap that is missing from medical schools and post-graduate CME, they will rapidly learn just how simple diagnosis is and how effective treatments are.
Confirming CIRS: Homing in on the case definition, what does potential for exposure mean? Potential for exposure demands objective findings showing microbial amplification with (1) visible mold; (2i) or presence of musty smells; (3) or determination of the types of molds found by DNA testing. We now add measurements of endotoxins and actinomycetes in modern labs with top-flight molecular methods to diagnostic criteria as these sophisticated assays are now readily available. Remember that musty smells, usually stemming from geosmin made by actinomycetes and occasionally by bacteria, are often used (curiously) to support a diagnosis of a mold problem. Use of accurate mold specific QPCR testing is readily and inexpensively available.

Unfortunately, some practitioners still think that air sampling has a role in the medical work-up of CIRS patients. Use of air samples for diagnosis is worse than worthless in that sampling air for spores, at least three microns in diameter or greater ignores 99.8% of the total amount of fragments that cause inflammatory responses! These fragments are so small they pass right through the spore trap devices. Spore trapping then can’t possibly be used to look for disease-causing inflammation. Don’t forget, exposure to small particles, really just biochemicals, means that the bulk of bad actors in WDB are not alive. Please don’t tell me to remediate a damp home by killing spores!
Even though spore sampling provides flawed information, that procedure is still widely used. Even worse than wrong-headed data generated by spore traps is the problem that occurs when people believe that spore trapping makes sense and that spore counts are indicative of something real in nature. Of note, air samples (1) only done for 5 or 10 minutes in a single-center location in a room do not tell us what has happened to bacteria or fungal spores that have settled out before the sampling; (2) don’t tell us what particulates were missed by sampling in the center of a room and not in boundary layers on the bottom and sides of a room; (3) do not separate benign versus pathogenic species of both Aspergillus and Penicillium (these two very large genera are lumped as Asp/Pen!); (4) will rarely show presence of heavier particulates such as those made by Stachybotrys; (5) will never show presence of xerophilic organisms such as Wallemia sebi; and (6) without repetition of air sampling findings, multiple times per day in a given room for each of multiple days per week, multiple weeks per month and multiple months per year, the World Health Organization has declared that air sampling is of no benefit.10

One reason for the commonality of microbial findings in water-damaged buildings being similar in each of our states, together with foreign countries, is that the indoor ecosystem of a wet building is uniquely similar across all climates. There rarely is any wind, and there certainly is not any rain or frozen precipitation. There is only a narrow range of temperature in an occupied building and only limited diversity of visiting or exotic organisms will be found. Often there will be limited movement of fixed objects in a room, setting up areas of reduced ventilation (“still air”). Fixed walls (not to mention floors and ceilings) create boundary layers of both air and particulates.
MSQPCR (Mold Specific Quantitative Polymerase Chain Reaction) is a marker of presence of different species of filamentous fungi found inside homes, both water-damaged and not. The fungal DNA present tell us much about the activity of water found inside the building. The EPA-developed ERMI (Environmental Relative Moldiness Index) purports to quantify an index of microbial contamination in a building from assessment of MSQPCR measured on dust samples. Initially done on vacuumed samples, ERMI was done later using Swiffer cloth wipe samplings, with comparable validity comparing Swiffer to vacuum.
Proper ERMI testing demands accurate use of high-quality probes and primers for detection and reporting. Laboratories that license the ERMI technology from the EPA must be able to show accurate and ongoing quality control. Never send a sample off to a lab that does not have ongoing EPA licensing, as errors are routinely seen with faulty use of primers or inexpensive, inadequate reagents. If a MSQPCR lab won’t tell you the quality control methods they use over the phone, don’t use it.
A lab test far more useful than ERMI and more accurate as a measure to show risk of recrudescence with re-exposure of CIRS patients to WDB is the Health Effects Roster of Type Specific (Formers) of Mycotoxins and Inflammagens, Version II (HERTSMI-2). HERTMSI-2 has been in increasingly wide use since its inception in 2011. Its accuracy is based on sorting health abnormalities associated with exposure to WDB to yield five species of fungi that (1) “span the globe,” of A(w) from the driest to the wettest organisms; and (2) show the overwhelming increase in CIRS when these specified organisms are found. By relying on correlation of spore equivalents/mg dust with risk of acquisition of adverse human health effects, we finally have a measure that predicts safety (or not) for over 95% of CIRS patients entering schools, workplaces and residences.
We need to remember that MSQPCR will not report bacteria, endotoxins, mVOCs or any other of the inflammagens found in WDB.
The scoring system for HERTMSI-2 weighs severity of contamination from 0-10 points for given organisms. When we sort these organisms by A(w), we find that the drier-loving species of Wallemia and Aspergillus penicillioides are routinely found in A(w) of 0.65-0.8 but are rarely represented by air samples. The common species of Aspergillus versicolor, usually found in higher A(w) of 0.8 to 0.9, are reported by ERMI but are never reported at the species level by spore traps. Presence of Chaetomium and Stachybotrys reflect environmental conditions with an A(w) of 0.9-1.0 are only detected infrequently in air samples using spore traps.
A word regarding dust collection. Swiffer cloths and vacuum samples are equally useful. If you use a Swiffer cloth, routinely available in a grocery store, use a new Swiffer, one cloth per sample. Put a glove on your left hand and wipe in one direction, either left to right or right to left. Use one cloth for all the sampling. We want you to sample for dust on the back of a shelf and not on the front where it might be more commonly dusted. Don’t use window sills or “public” areas, like hallways. I suggest avoiding shoes on closet floors, but closet shelves are fair game. Bathrooms are best avoided because of the role of water saturation following showers or bathing. If there is evidence of obvious microbial growth, resist the temptation to swipe it, as sampling the black patch on the bedroom wall, for example, will skew your sample to render results less reliable. If there is a crawlspace or a sump pump or a basement or an indoor spa or areas in bathrooms that are hampered by low air flow with inadequate exhaust, be sure to test for endotoxins with the same sample used for HERTMSI-2. Testing for abundance of Actinomycetes species is of tremendous value, especially when Aspergillus penicillioides or Wallemia are predominant. This is not to say that actinomycetes won’t grow in wetter environments, but they are more commonly found in drier environments indoors. They also like more alkaline surfaces like concrete that is chronically moist.
We have seen that the causation of illness from water-damaged buildings is multi-factorial. We can’t just rely on fungal DNA because in a way, what we are asking is, “Can we identify specific (only one thing causes the illness) causation of human illness found from water-damaged buildings?” The answer is NO!
Countless different measurements, mostly not available (think about spirocyclic drimanes, known to cause inflammation but for which there are no commercial test available), are needed for 100% surety. We are less able to measure beta glucans and mannans. Moreover, microbial V0Cs are showing great potential to be a biomarker for water-damage, but the human health effects data associated with mVOC exposure is not confirmed. Please note that transcriptomics is changing the “no specific causation” idea. Differential gene activation can tell us if it is likely that reactivity to mycotoxins, actinomycetes, or endotoxins has occurred.
Symptoms
When we look at specific symptoms in CIRS, using a list of 37 symptoms (the same symptoms as seen in Table I, but separated by organ system this time) that have been collated from charts of thousands of cases and each found in more than 30% of cases, we find fatigue and weakness together with headaches, aches, and muscle cramps, defining involvement of three separate organ symptoms. Unusual pains, sharp stabbing pains, clawing pains, electrical pains, comprise their own category (possibly due to activity of transient potential receptor vanilloid (TRPV) activity on sensory neurons). Here we will also find sensitivity to the light touch, especially from water droplets in a shower or rainstorm. Our ophthalmic findings (in addition to visual contrast sensitivity, VCS) are light sensitivity, redness, blurred vision, and tearing. Respiratory issues are shortness of breath, cough and sinus congestions; abdominal pains and secretory diarrhea comprise our abdominal findings. Musculoskeletal problems are quite common with joint pain, especially with morning stiffness, being routinely found in patients over age 25. Of note is that ESR is invariably low normal. Perhaps of greatest importance are the symptoms suggestive of brain injury with executive cognitive dysfunction represented by deficits in recent memory, concentration, difficulty with word finding, assimilation of new knowledge, confusion, and disorientation leading the list. If present, think “brain fog,” and get a NeuroQuant.
Hypothalamic symptoms include mood swings, appetite swings, unusual sweats, and difficulty with normal temperature regulation. Our renal findings are excessive thirst, frequent urination, and curiously, increased susceptibility to static shocks, but not just in dry environments. Neurologic findings of numbness, tingling, and taste abnormalities (metallic taste, especially) are common in CIRS. Additional neurologic problems include vertigo and skin tremor (get a NQ!).
Given that symptoms and VCS taken together (see cluster analysis, Table 1) are so accurate, one might reasonably ask, “Why do we need laboratory findings?” The answers are straightforward: (1) we must have an accurate ongoing differential diagnosis; (2) laboratory changes will show interval improvement with therapy or worsening with re-exposure (often not obvious!); (3) findings objectively demonstrate the physiology to interested third parties; and (4) provides opportunity for further study.
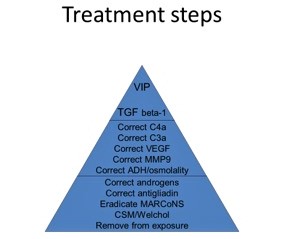
Figure 2 is the Treatment Pyramid. The Treatment Pyramid has also stood the test of time with a 12-step protocol providing predictable improvement as shown in at least 30 countries around the world and in all 50 United States.


Ritchie C. Shoemaker, MD, remains active in the field of biotoxin-associated illnesses, the focus of his practice since 1997. At that time, an outbreak of unexplained human illness, associated with exposure to blooms of a dinoflagellate, Pfiesteria piscicida, attracted his attention and interest. Pfiesteria was the first example of an acute and then chronic biotoxin-associated illness recognized and published in peer reviewed literature. Shoemaker’s two papers on diagnosis and then treatment were the first in the world’s literature on acquisition of illness from Pfiesteria in the wild. Since that time, other sources of biotoxin associated illnesses have come forward including other dinoflagellates, cyanobacteria and, most importantly, organisms resident in water damaged buildings. Shoemaker has spent the last 22 years treating patients and conducting research that unveils the extraordinary complexity of these illnesses, now called chronic inflammatory response syndromes (CIRS). Starting with no biomarkers and now progressing to over 25, CIRS has been shown to have abnormalities in proteomics and transcriptomics with differential gene activation, the final ultimate pathway of disease production in the world of chronic fatigue.
His collaboration with Dr. James C Ryan, transcriptomist, has led to multiple publications that have application, not just to chronic fatiguing illnesses but to the inflammatory illnesses of the 21st century including atherosclerosis, diabetes, obesity, and autoimmune illness.
As Shoemaker’s work has progressed on the complex problems of grey matter nuclear atrophy, a small but growing cohort of patients with multinuclear atrophy and cognitive impairment have led to improvements that may have application to illnesses such as Alzheimer’s disease.
References
1. Berndtson K, McMahon S, Ackerley M, Rapaport S, Gupta S, Shoemaker R. Medically sound investigation and remediation of water-damaged buildings in cases of CIRS-WDB. Part 1. (Table 2) 10/15. www.survivingmold.com. Accessed 7/23/2017.
2. Shoemaker R, Heyman H., Annalaura M, Ryan J. “Inflammation Induced Chronic Fatiguing Illnesses: A steady march towards understanding mechanisms and identifying new biomarkers and therapies.” Internal Medicine Review 3.11 (2017): 1-29.
3. McMahon S, Kundomal K, Yangalasetty S. Pediatric norms for VCS testing using an APT VCS tester. MRA 2017; 5: 1-7.
4. Keller B, Pryor J, Giloteaux L. Inability of myalgic encephalomyelitis/CFS patients to reproduce VO2 max peak indicates functional impairment. J Transl Med 2014; 23: 12.
5. Shoemaker R, House D, Ryan J. Vasoactive intestinal polypeptide (VIP) corrects chronic inflammatory response syndrome (CIRS) acquired following exposure to water-damaged buildings. Health 2013; 5(3): 396-401.
6. Shoemaker R, House, D, Ryan J. Neurotoxicology and Teratology doi: 10.1016/j.ntt.2014.06.004. Structural brain abnormalities in patients with inflammatory illness acquired following exposure to water-damaged buildings: A volumetric MRI study using NeuroQuant.
7. McMahon S, Shoemaker R, Ryan J. Reduction in Forebrain Parenchymal and Cortical Grey Matter Swelling Across Treatment Groups in Patients with Inflammatory Illness Acquired Following Exposure to Water-Damaged Buildings. J Neurosci Clin Res. 2016; 1(1):1-11.
8. Shoemaker R, Katz D, Ackerley M, Rapaport S, McMahon S, Berndtson K, Ryan J. Intranasal VIP safely restores atrophic grey matter nuclei in patients with CIRS. Internal Medicine Review 2017; 3(4): 1-14.
9. Shoemaker, R. 5/4/2018 Conference proceedings; Surviving Mold, Salisbury, Md. MARCoNS monsters, antifungals and grey matter atrophy.
10. Afshari A, Anderson HR, Cohen A, de Oliveira Fernandes E, Douwes J, Gorny R, Hirvonen M-R, Jaakola J, Levin H, Mendell M, Molhave L, Morwska L, Nevalainen A, Richardson M, Rudnai P, Schleibinger HW, Schwarze PE, Seifert B, Sigsgaard T, Song W, Spengler J, Szewzyk R, Panchatcharam S, Gallo G, Giersig M, Nolokke J, Cheung K, Mirer AG, Meyer HW, Roponen M. (2009). World Health Organization guidelines for indoor air quality: dampness and mould. WHO guidelines for indoor air quality.



