|
Page 1, 2, 3
At What Age Does Testosterone Deficiency in Men Start, and Should It Be Treated?
Testosterone deficiency may occur at any age. Even a male newborn may be deficient in testosterone. If male babies do not present a higher peak of testosterone in the blood at birth and during the 2 months that follow, they may suffer from genital underdevelopment.1,2 Cryptorchidism and less "masculine" behavior in boys may reflect very early testosterone deficiency. Adolescents and young adults may be testosterone deficient too, suffering from muscle, body hair, and beard underdevelopment as a result.
In most men, testosterone deficiency appears at a later age. The highest testosterone levels are found at ages 18 to 25. After age 25, testosterone levels slowly decline, especially intracellular testosterone levels.3
Why? There are several reasons. First, as an autopsy study showed, the total number of testosterone-producing Leydig cells decreases in adult men from age 18 on. A man goes from having an average of 7 million young and well-working Leydig cells at age 18 to just 2 million old and dysfunctional Leydig cells at age 80. That is a reduction by more than 70%!4 This decline corresponds to a definitive net loss of 1 testosterone-producing Leydig cell every 4 to 5 minutes on average. Of course, new Leydig cells are formed daily, but after age 25, over time, more Leydig cells disappear than new ones appear.
If you read this article carefully, it might take you 20 to 25 minutes. In that time, the average male reader loses 4 to 5 Leydig cells. (Of course – or at least I hope – it is not due to the reading of this article, as reading other similar-length articles should provide an equivalent loss in Leydig cells.)
Second, Leydig cells decline not only in number but also in function and efficacy with age, so each remaining Leydig cell experiences increasingly greater difficulties with producing testosterone. The remaining Leydig cells at ages 40, 60, or 80 will not produce as much testosterone as an equivalent number of cells at age 18 would.5
Speed of loss of testosterone-producing Leydig cells from age 18 to 804:
115,000 Leydig cells net loss per year
300 Leydig cells net loss per day
15 Leydig cells net loss per hour
1 Leydig cell net loss every 4–5 minutes |
Third, the gradual age-related decline in the serum testosterone level worsens by a progressive increase in the serum level of sex hormone-binding globulin (SHBG), the protein that transports testosterone in the blood from the testicles to the target cells. The higher the SHBG level, the more testosterone remains sequestrated in blood, tightly bound to SHBG, and the slower and less testosterone (molecules) penetrates the target cells to express their action. The decrease in testosterone bioavailable for the target cells shows up by an age-related decrease in serum-free testosterone levels that is greater than the decline in total (free + bound) testosterone.6
Fourth, the target cells for testosterone also age. They react less efficiently to testosterone. This decline in target-cell sensitivity is due to several factors: a decrease in the number and quality of its intracellular testosterone receptors, the accumulation of waste products inside the target cells that hinder metabolic activities, a decrease in functional enzymes to express the effects of testosterone, and so on.7
Fifth, as a consequence of previous disorders, the testosterone metabolic effects on the male body gradually decline with age. In laboratory tests, a decrease in testosterone metabolites reflects this decrease in testosterone action.8-10 A testosterone metabolite is obtained each time a testosterone molecule reaches and binds to a testosterone receptor in the nucleus of a target cell, and it starts the chain of metabolic reactions leading to a testosterone effect. During this interaction, the testosterone molecule becomes converted into a testosterone metabolite. The testosterone metabolites androsterone and etiocholanolone can be measured in 24-hour urine, while the best androgen metabolites in the serum to assess are dihydrotestosterone and androstanediol glucuronide, which concentration is on the average double that of testosterone.8-10 The decline in testosterone metabolites is greater than the decrease in the free and total testosterone levels in the serum.
The gradual drop in the serum, urinary, and tissue levels of testosterone and its metabolites, and the consequent drop in the testosterone psychological and somatic effects, beginning at ages 25 to 30, suggest that most men aged 30 to 40 start to suffer from symptoms and signs of testosterone deficiency that are sufficient to justify testosterone supplementation, at least a low dose.
Who is Affected by ADAM or PADAM Syndrome?
Testosterone deficiency due to the progressive age-related decline in testosterone levels and its effects has received names such as the ADAM (androgen deficiency in aging males) syndrome or PADAM (partial androgen deficiency in aging males) syndrome.11 The term aging males is misleading, as for most people, aging starts around age 45 to 50 or even 60, while in reality, testosterone deficiency due to aging starts at a much younger age, from 25 to 30. At age 30 and over, the PADAM syndrome becomes apparent by slight, almost unapparent, declines in male characteristics.
Testosterone, the Male Hormone
Testosterone, also called the "male hormone," is the true key to masculinity. It is the hormone that makes a man a real man. Any decrease in testosterone level brings a decrease in manhood, an unbearable thought for some men. To avoid this unnecessary suffering, testosterone levels can be kept at a sufficient level for a man to keep his masculine effects.
The Real Significance of the Reference Limits and Interval for Testosterone
Many physicians erroneously consider the lower reference limits for total and free testosterone in the serum as thresholds below which there is testosterone deficiency, but above it is OK for them. However, the lower limit, just as the upper reference limit for testosterone, is not a health limit separating healthy and unhealthy testosterone levels. No, the lower reference limit is a purely statistical limit which tells us that 2.5% of male patients who get their testosterone checked at the laboratory have testosterone levels below this limit. A total of 95% of all other male patients will statistically present testosterone levels within the reference interval, between the upper and lower reference limits, while 2.5% have levels above the upper limit.12 In no way does the lower testosterone reference limit signify that only the 2.5% of patients below this threshold are the ones who are testosterone deficient! Dogmatically relying on these limits to decide whether a testosterone level is healthy or not is a mistake, one that physicians make too often.
What Is the Frequency of Testosterone Deficiency in Men?
Almost every man aged 30 or over undergoes a slow and progressive decline in testosterone levels. The drop is often barely visible in the beginning and so slow to develop that many men become aware of it only at a far advanced age, 50 or over, when many disorders facilitated by the testosterone deficiency, such as abdominal obesity and cardiovascular disease, may have developed. This could have been prevented by an early testosterone treatment started between ages 30 and 40.
Adverse Consequences of Testosterone Deficiency at Testosterone Levels Still Within the Reference Range
Small drops in testosterone levels of 10% to 20% within the reference range may pave the way for the development of the first complaints and physical signs of testosterone deficiency.
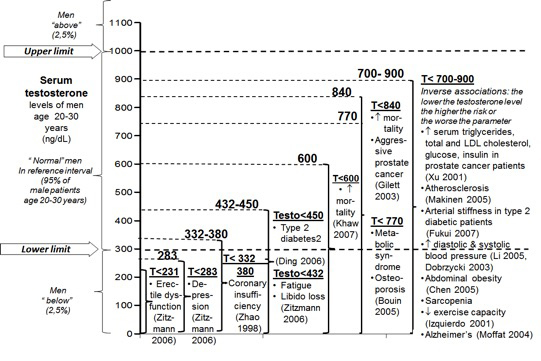
Research investigations have shown that men with testosterone levels situated in the lower 25%, 33%, 50%, or even 66% of the reference range are at higher risk of developing obesity, metabolic syndrome, diabetes, bone density loss, sarcopenia, dyslipidemia (high serum levels of triglycerides, lipoprotein a, apoB 100, LDL and total cholesterol and high HDL cholesterol), atherosclerosis, arterial hypertension, heart disease – especially coronary heart disease, cognitive dysfunction, including Alzheimer's disease, prostate cancer, in particular aggressive prostate cancer, and premature death.14-53 According to these studies, 25% to 66% of men aged 30 or older have testosterone levels within those lower portions of the reference interval that are too low to ensure optimal health. The occurrence of these increased risks at these testosterone levels within the reference range strongly suggests that at these levels an intermediate degree of male hormone deficiency, which requires testosterone treatment to revoke the risks, has developed. These studies confirm the inadequacy of considering the lower and upper reference limits for testosterone as sharp limits between health and illness.
The figure below provides an overview of testosterone levels below which there are statistically significantly higher risks of disease and mortality.
The 'Optimal' Testosterone Level
The data on the adverse health effects of lower (and average) serum testosterone levels within the reference range shown in the above-mentioned figure suggest that the "optimal" serum (total) testosterone level of the average man should be at or – even better – slightly above the mean level of young adults (ages 18 to 30). Thus, the "optimal" testosterone serum level would be 650 to 850 pg/mL (or 6500 to 8500 pg/mL, or 22.5 to 29.5 nmol/L). This concentration should correspond to the patient's highest testosterone level as a young man.
However, these optimal testosterone levels are merely indicative. Taller and more muscular men need higher testosterone levels, as they have built their bodies on higher testosterone levels in young adulthood. They need to keep their levels higher throughout their lives to maintain their bodies' health. Small-sized and thin-muscled men often feel best at lower levels of testosterone, below the average level of young men, because they have always had below-average testosterone levels that fit their body types. Even so, the testosterone level they need to feel best is still (much) higher than the lower reference limit.
What Are the Benefits of Testosterone for Men?
Testosterone is best known as the male sex hormone that stirs men's sex drive and improves their erectile function, but testosterone produces many other beneficial effects.54-56
 Testosterone is the hormone for the muscles. A healthy body is a firm body with toned muscles partly due to the correct level of testosterone. In contrast, the typical lax and slumped bodies seen in most men of advanced age are typically testosterone-deficient bodies. The appearance of excess fat and loose muscles indicates that a man's health has declined, partly due to testosterone deficiency. Testosterone has anabolic effects on all types of muscles, not only on the biceps or abdominal muscles. It also builds up the heart, which is mainly made of muscle fibers, and the arteries, each of which is essentially made of a thick layer of smooth muscles, except for a thin inner layer of endothelial cells. A lack of testosterone facilitates the development of atherosclerosis, including coronary insufficiency, by letting the arteries prematurely age.57-59 Testosterone treatment reverses this condition.60 Testosterone deficiency is also associated with an increased risk of heart disease due to fiber muscle atrophy of the heart muscle Testosterone treatment reduces the myocardial ischemia and cardiac dysfunction in male coronary heart disease patients.61,62 Testosterone is the hormone for the muscles. A healthy body is a firm body with toned muscles partly due to the correct level of testosterone. In contrast, the typical lax and slumped bodies seen in most men of advanced age are typically testosterone-deficient bodies. The appearance of excess fat and loose muscles indicates that a man's health has declined, partly due to testosterone deficiency. Testosterone has anabolic effects on all types of muscles, not only on the biceps or abdominal muscles. It also builds up the heart, which is mainly made of muscle fibers, and the arteries, each of which is essentially made of a thick layer of smooth muscles, except for a thin inner layer of endothelial cells. A lack of testosterone facilitates the development of atherosclerosis, including coronary insufficiency, by letting the arteries prematurely age.57-59 Testosterone treatment reverses this condition.60 Testosterone deficiency is also associated with an increased risk of heart disease due to fiber muscle atrophy of the heart muscle Testosterone treatment reduces the myocardial ischemia and cardiac dysfunction in male coronary heart disease patients.61,62
Testosterone also makes bones stronger and denser with a higher mineral content.63,64
Next to cardiovascular diseases, testosterone has also been reported to reduce the occurrence and severity of age-related diseases, such as obesity, diabetes, osteoporosis, and Alzheimer's disease. 65-73
Mentally, testosterone improves memory by increasing the number of synaptic connections between neurons and by thickening the myelin sheaths around the axons in animals. 74-76 It does not however, increase the number of neurons.76 This means that testosterone helps individuals to understand complex information more easily. Emotionally, testosterone improves mood, makes men courageous, and may help to reduce depressive states, such as those experienced by men around age 40 or those that do not respond to antidepressants, although results for depression are not always consistent.77-81
Finally, several scientific studies have shown in men that increasingly testosterone treatment of men with low testosterone level reduce the risk of premature death.82,83
Page 1, 2, 3
|




