|
A Multifocal Strategy for Cancer Control
Cancer can be - and often is - a wily opponent. In large measure, this reflects the fact that it is a constantly moving target. Cancer is heavy-handed. There is nothing subtle at all about the presence of a malignant tumor in your kidney or lung. Cancer makes no attempt to veil its threat. It is a disease that can gather momentum quickly and attack with frightening ferocity. Only a concerted and combined effort can repel such an attack. It is necessary to combat it from every possible angle.
Our total-care approach requires the patient's full participation. C
ancer treatment is not a spectator sport. The patient must be prepared for the fight. We go through a process of structuring a patient for success by providing the necessary resources to face the threat at the physical, emotional, and spiritual levels. There is no question that the alliance between body, mind, and spirit can even the playing field against cancer.
In addition, it is important to remember that the ultimate goal when treating advanced stage IV cancer is to insure that patients can enjoy a reasonably high quality of life during the months and years that they are fighting their cancers.
The Oasis of Hope IRT Protocols
Cancer patients in stage IV were enrolled into one of our two main protocols, known as "IRT-Q" and "IRT-C." Although these protocols share many common features, they are differentiated by the fact that patients on the IRT-Q protocol receive chemotherapy, whereas those on the IRT-C protocol do not, but rather receive extra infusions of high-dose intravenous vitamin C as an alternative approach to attacking the cancer. Patients on each protocol receive a range of additional interventions, including oxidative preconditioning therapy, redox regulatory therapy, cell signal transduction modulatory therapy, metronomic chemotherapy, cancer-retarding anti-inflammatory therapies, optimal diet and exercise, and emotional and spiritual support.
Killing the Cancer Cells with Chemotherapy: The IRT-Q Protocol
For some types of advanced cancer, specific chemotherapy drugs are known to have at least some efficacy in a high proportion of cases - especially if the patient has not received that drug previously. For patients who fall into this category, and whose physical condition makes chemotherapy feasible, Oasis of Hope physicians usually recommend an IRT-Q protocol. (The Q reflects the fact that the Spanish word for "chemotherapy" is quimioterapia). Patients enrolled in an IRT-Q protocol visit the clinic at least three times for a course of appropriate chemotherapy. The chemotherapy regimens employed at Oasis of Hope - usually first-line chemotherapy - are well documented in the credible medical literature, and are used in the full doses shown to have potential efficacy.
But what sets Oasis of Hope apart from many other clinics employing chemotherapy is our use of many adjuvant measures intended to make the chemotherapy more effective at killing the cancer cells, while simultaneously minimizing the damage done to healthy tissues.
Coping with Tumor Hypoxia
One way to make chemotherapy more effective is to insure that cancer cells are adequately oxygenated. Because tumors tend to have haphazard blood supplies, some parts of tumors tend to receive relatively little blood flow and are thus poorly oxygenated (hypoxic). For reasons that are not yet entirely clear, hypoxic cancer cells are often harder to kill with chemotherapy or radiotherapy. So we use several strategies for improving the oxygenation of tumors. Prior to the administration of chemotherapy, patients are infused intravenously with a perfluorocarbon polymer called "Perftec"; this is an oxygen (O2) carrier that complements the ability of red blood cells (RBC) to deliver O2 to the tumor. Because the particles of Perftec are so much smaller than RBC, they can flow through constricted capillaries that would exclude RBC. The oxygen-carrying capacity of Perftec is boosted by having the patients breathe oxygen-enriched air when chemotherapy drugs are subsequently administered.
Another way in which we improve tumor oxygenation is by administering ozone-autohemotherapy (O3-AHT) prior to chemotherapy; this strategy has been shown to make RBC more flexible and blood less viscous, and its oxygenated RBC surrender O2 to tissues more readily (rightward shift of dissociation curve); also, it promotes vasodilation by stimulating nitric oxide release by the endothelial lining of small arteries.1 The net result is more O2 delivery to the hypoxic tumor regions.2,3 Recently, researchers at the Canary Islands Institute for Cancer Research recruited 18 cancer patients and used special needle probes to measure the O2 content of their tumors before and after 3 sessions of O3-AHT; they were in fact able to establish that there were fewer hypoxic tumor regions following O3-AHT.2
Oasis of Hope has also developed a novel strategy for increasing the chemosensitivity of cancer cells that nevertheless remain hypoxic. Recent research demonstrates that hypoxia protects tumor cells, at least in part, by diminishing the capacity of these cells to produce an intracellular signaling factor known as cyclic GMP (cGMP). Prior to chemotherapy, we administered high oral doses of the B-vitamin biotin; in high concentrations, biotin has been shown to directly stimulate cGMP production, both in tumors and healthy tissues. (Fortunately, increased cGMP doesn't seem to influence the chemosensitivity of cells that are well oxygenated, so biotin shouldn't boost the chemosensitivity of healthy tissues.)
Chemosensitizing Agents
Recent rodent research shows that high but tolerable intakes of the antioxidant nutrient selenium can boost the chemosensitivity of many types of cancer - while at the same time making healthy tissues more chemoresistant. We employed high-dose selenium supplementation prior to and during chemotherapy. Another agent that boosts the chemosensitivity of many cancers is the activated metabolite of vitamin D3.
In many cancers, their relative chemoresistance reflects increased intracellular activity of a factor known as NF-kappaB. Since the natural drug salicylate and the herbal compound silibinin have shown the capacity to inhibit NF-kappaB activity in clinically feasible doses, these agents are also employed as chemosensitizing agents in the IRT-Q protocols.
Other agents that have potential for chemosensitizing certain tumors and are often administered in conjunction with chemotherapy at Oasis include boswellic acids and the drug diclofenac. Suffice it to say that we spare little effort to insure that the chemotherapy which we employ will kill as many cancer cells as is physically possible!
Protecting Healthy Tissues
One reason why our IRT-Q protocol is gaining increased popularity with our patients is that we incorporate several measures to protect healthy tissues - thus making chemotherapy a less traumatic experience. The O3-AHT mentioned above has a dual purpose; in addition to improving tumor oxygenation, it also provides "oxidative preconditioning." The chemically altered compounds in ozonated blood are "perceived" by healthy tissues as a sign of oxidative stress; in response, these tissues boost their production of antioxidant enzymes and other protective factors. This procedure is typically repeated 4 to 5 times during the week before chemotherapy to provide an oxidative tolerance state in the patient. Then, when chemotherapy is subsequently administered, these tissues are better able to cope with the pro-oxidant activity of these cytotoxic drugs, so that they are less damaged. This translates into less bone marrow damage, less nausea, and fewer side effects of other kinds.
As noted, the high-dose selenium employed with IRT-Q has the potential to protect normal tissues. Another component of IRT-Q that is protective in this regard is the hormone melatonin, which mitigates chemotherapy-induced damage of the bone marrow. And supplementation with the amino acid glutamine, a key source of calories for cells in the intestinal tract, is employed to reduce damage to these cells. Also, silibinin has the potential to protect the liver.
An Alternative Strategy for Killing Cancer: IRT-C
Some types of cancer are so poorly responsive to available chemotherapeutic drugs that chemotherapy is considered inadvisable. Moreover, even when a patient has a type of cancer that is potentially susceptible to chemotherapy, his or her current clinical condition (bone marrow depression, bile duct blockage, etc.) may make chemotherapy currently inappropriate. And some patients simply refuse to accept chemotherapy. For patients who fall into this category, Oasis of Hope used an alternative protocol known as IRT-C.
Oxidizing Cancer to Death
A high proportion of cancers have low activity of the enzyme catalase, which degrades the oxidant chemical hydrogen peroxide (pO2).4,5 This adaptation may be beneficial to the cancer; although oxidant chemicals can be toxic to cells, moderate increases in oxidant stress aid the growth and survival of many cancers.6,7 However, low catalase makes cancers potentially vulnerable to attack with pO2. Recently, researchers at the National Institutes of Health have discovered that high concentrations of vitamin C can react spontaneously with molecular oxygen within tumors to generate large amounts of pO2, which can be lethal to tumor cells whose catalase activity is low.8,9 Such large concentrations can only be achieved by high-dose intravenous infusions of vitamin C - oral administration is ineffective in this regard.10 These findings rationalize several previous case reports of objective tumor regression in cancer patients treated repeatedly with high-dose intravenous vitamin C.11-13 The vitamin C is not toxic to normal healthy tissues, because they have ample amounts of catalase activity. Our current protocol insures that blood and tissue levels of vitamin C will remain high (millimolar levels, close to those of blood sugar) for at least 4 hours.
Vitamin K3 as an Adjuvant
The ability of vitamin C to generate pO2 in tumors apparently hinges on the presence of unknown catalysts that can transfer electrons from vitamin C to O2 molecules, generating the unstable compound superoxide.8,9 The latter is rapidly converted to pO2, which can move into cancer cells, and mediates the tumor cell death achieved with successful vitamin C therapy. Dr. Mark Levine, whose research encouraged us to develop our IRT-C protocol, speculates that extracellular protein-bound iron serves as this catalyst.9 It is conceivable that the availability of this catalyst might vary from tissue to tissue and person to person, depending on nutritional status or genetics. Furthermore, there is no reason to assume that levels of this catalyst are sufficient to permit an optimally intense generation of pO2 in tissues.
Certain small soluble organic molecules can perform the same catalytic function, expediting the transfer of electrons from vitamin C to O2. In particular, menadione - also known as vitamin K3 - has this capacity.14 And menadione may be particularly appropriate for this purpose, as it has long been in clinical use as a source of vitamin K activity.15
There is a substantial research literature demonstrating that joint incubation with vitamin C and menadione is often selectively toxic to cancer cells.16,17 Researchers at the Catholic University of Louvain, Belgium, demonstrated the potential utility of vitamin C/menadione in cancer therapy. They report that this therapy is well tolerated, without any evident damage to healthy tissues. They also demonstrate that vitamin C/menadione can interact synergistically with certain chemotherapy drugs in killing cancer cells, presumably because a concurrent increase in oxidative stress can make these drugs more lethal.18 This observation has been independently confirmed.19 Indeed, there are reports that menadione alone can potentiate the cancer-killing action of certain chemotherapy agents, presumably because, in sufficiently high concentrations, intracellular menadione can generate oxidative stress by transferring electrons from intracellular molecules O2.20,21
The inclusion of menadione in our vitamin C infusions markedly potentiates generation of pO2 in tumors, enabling a more substantial cell kill in those cancers that are sufficiently low in catalase activity.
In patients whose tumors are potentially responsive to chemotherapy but whose physical condition is not yet ready to tolerate it, IRT-C often provides enough tumor control to give their normal tissues a chance to heal, so that they again become appropriate candidates for chemotherapy.
Tumor Oxygenation: Ozone and Perftec
However, this strategy can only work well in tumors that have adequate levels of O2, as vitamin C reacts with O2 to produce the pO2. Portions of many tumors tend to be low in O2 (hypoxia), as the blood flow through tumors is often sluggish compared with that which supplies normal tissues; this evidently could compromise the antitumor efficacy of vitamin C therapy. To overcome this problem, we employed several complementary techniques that can boost the O2 content of tumors: Perftec and O3-AHT. The combination of O3-AHT and Perftec infusion can be expected to improve O2 availability in hypoxic regions of tumors - which in turn should boost the ability of intravenous vitamin C and vitamin K to generate pO2 in tumors.
Concurrent Chemotherapy
Patients in the IRT-Q protocol received intravenous vitamin C infusions right after chemotherapy and on the following 4 days. There are reasons to believe that the oxidative stress induced by the vitamin C in the tumor, as well as the improved tumor oxygenation made possible by O3-AHT and Perftec, will often increase the ability of the administered chemotherapy drugs to kill cancer cells.22-25 The IRT-C protocol has been designed to exploit these complementary interactions, so that destruction of cancer cells can be maximized without increasing the toxic risk to healthy tissues.
Other Adjuvant Measures
We employed additional adjuvant measures that, in at least some tumors, are likely to potentiate the killing of tumor cells achieved through our vitamin C and K3/chemotherapy regimen. The natural compound salicylate - derived from white willow bark, which has been used for centuries as an anti-inflammatory therapy - can enhance the sensitivity of many tumors to chemotherapy and pO2 by inhibiting the activity of NF-kappaB; this factor is activated in a high proportion of advanced cancers, and works in multiple ways to render these cancers less sensitive to chemotherapy and oxidative stress.26-29
Prior to receiving vitamin K3 and vitamin C (and possibly chemotherapy), patients are also supplemented with selenium and silymarin (a source of the natural anti-inflammatory compound silibinin). Like salicylate, these agents have potential for sensitizing tumors to killing by chemotherapy or oxidative stress. Silymarin's activity in this regard may be similar to salicylate's: it suppresses activation of NF-kappaB.30,31 Recent studies show that high doses of organic selenium can make cancer cells more sensitive to many types of chemotherapeutic drugs; there are reasons to believe that selenium may also make pO2 more lethal to tumors. We also used high doses of vitamin D3 - as a chemosensitizing agent.32
Patients were also be supplemented with various nutrients - such as fish oil, green tea polyphenols, and melatonin - whose purpose is to slow tumor growth by blocking new blood vessel formation (angiogenesis) or boosting the body's immune capacities. Supplementation with these nutrients will continue after patients return home between hospital therapy sessions; this "after-therapy" can be crucial for improving chances of a cure or at least achieving a worthwhile prolongation of high-quality life.
Oasis of Hope At-Home Therapies
With most chemotherapies, it is necessary to give the body at least a few weeks to heal before another course of chemotherapy is administered. So Oasis of Hope patients went home for several weeks in between courses of chemotherapy. We provided an elaborate at-home therapeutic regimen, the intent of which is to slow the grow-back of the remaining tumors between sessions of chemotherapy. On the other hand, chemotherapy may have a chance to induce a substantial remission if each course kills a significant number of cells, and grow-back between chemo sessions is slow.
Patients in the IRT-C protocol also return home for several weeks between their courses of vitamin C infusions. They receive a similar at-home therapeutic regimen as patients receiving IRT-Q. The rationale of the at-home therapy in IRT-C is the same - to slow the grow-back of tumor between sessions of in-hospital vitamin C infusions.
The therapeutic strategies described here are also employed in the long-term follow-up (or maintenance) therapy prescribed for Oasis of Hope patients after they have completed an IRT-Q or IRT-C protocol. The intent here is to slow the growth of residual tumor, postponing as long as possible the need for further cancer-killing therapies.
The tumor-retardant strategies employed in the at-home regimens have several goals:
- to slow tumor growth by intervening directly in signaling pathways that make cancer grow more rapidly and aggressively; a number of nutraceuticals and drugs employed in both IRT regimens to slow tumor growth included salicylic acid (salsalate), silibinin, diclofenac (an inexpensive cox-2 inhibitor), boswellic acids, vitamin D, aged garlic extract, and (in prostate, colon, and ovarian cancers) soy isoflavones;
- to inhibit the angiogenic process that makes tumor spread possible by providing new blood vessels for the tumor; the nutraceuticals and drugs employed to slow angiogenesis include green tea polyphenols, the amino acid glycine, salsalate, silibinin, diclofenac, vitamin D, and fish oil;
- to boost the immune system function by activating the natural killer cells (NKC) to eliminate new small metastases or residual nests of cancer cells; the nutraceuticals and drugs employed are melatonin, selenium, diclofenac, and glutamine. Metronomic chemotherapy has a favorable impact on the capacity of NKC to attack cancer cells; it selectively eliminates a type of white cell called a Treg cell that suppresses the cytotoxic activity of NKC;
- to decrease risk for new metastases by intervening in the metastatic process; it has been shown that modified citrus pectin and cimetidine suppress this process;
- to minimize risk for cachexia, a common complication of tumor spread, entailing substantial loss of muscle mass. The substantial loss of muscle mass in cachexia reflects an inflammatory reaction in skeletal muscle fibers that is much more severe than that loss of muscle mass seen with caloric restriction alone. To prevent cachexia we used salsalate, silibinin, melatonin, glutamate, and fish oil.
Addressing Psychological Factors
We included laughter therapy in the IRT protocols. We also have a lovely nondenominational chapel, and a pastor to whom patients have ready access. Religious-themed lectures stressing hope and compassion are often presented at Oasis, for the benefit of patients who have spiritual beliefs. Patients are encouraged to wear their regular clothes, to eat together in the communal dining hall where three quasi-vegan low-fat meals are served each day, and to develop friendships and share experiences with their fellow patients. Frequent communication between doctors and patients is also encouraged; every week there are IRT lectures and a question-and-answer session to answer any question that the patients care to ask about their therapy
Alteration of Lifestyle
While patients received treatment at Oasis of Hope, we educated them on how to live healthful lives when they returned home and how to continue therapy. Our doctors and nurses worked with patients and their loved ones to teach them how to effectively self-administer therapies. This is a very cost-effective way for patients to continue therapy for a prolonged period of time.
We observed that the patients who get the best results are those who make a real commitment to the program, the ones who have the discipline and desire to adhere to the therapies prescribed. A tragic error that many patients make is to abandon therapy as soon as they start to feel better or when they experience remission. Those who continue therapy, adhere to the nutrition program, take the nutraceuticals from the at-home program, and come back for the maintenance treatments and the follow-up program gain the best results.
The follow-up program lasts a full five years at no additional cost to the patient. At these follow-up visits, all the doctors monitor the patient's progress and make any modifications to the home therapy that will better meet the patient's health-care needs. We believe that the periodic phone calls which we make to the patients have been vital because people need the encouragement and to know that their doctor really cares.
We encourage every patient to completely adhere to the therapies and embrace the lifestyle changes that we recommend at Oasis. We believe that a patient's commitment to the therapy is the single most important factor that determines how effective treatment is.
IRT Survival Rates
The Oasis IRT-Q regimen has been in place sufficiently long that we can now calculate 5-year survival statistics for a group of patients who have received this treatment for breast (45 patients), ovarian (15 patients), lung (23 patients), and colorectal cancer (25 patients). And 4-year survivals can be calculated for patients with these cancers who have received the IRT-C protocol. Since most patients who come to Oasis have advanced metastatic disease when they get here, we have restricted this analysis to patients who were stage IV at the time of diagnosis, so that Oasis's results can be compared objectively with those of other medical centers. (Stage IV usually means that metastases are present in distant organs.) Also, we have included only those patients who were sufficiently healthy to complete at least 3 courses of therapy, which usually takes about 4 months. In patients diagnosed with stage IV breast cancer, we have also done a separate analysis for those patients who arrived at Oasis of Hope within 6 months of their diagnosis. For many of those, Oasis of Hope was their first treatment option.
Table 1 displays our IRT-Q results, side by side with the results of conventional US therapy. The results of "conventional treatment" which we have included for comparison are derived from the National Cancer Institute's recent (2007) SEER Survival Monograph: Cancer Survival Among Adults - U.S. SEER Program. This publication provides average cancer survival rates in major regions of the US.
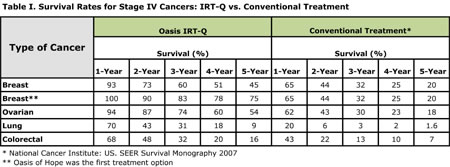
It is clear that, in terms of survival, Oasis patients who received IRT-Q are doing considerably better than those receiving the average standard of care in the US. In fact, 5-year survival in each of these cancers is at least 2- to 3-fold higher than in patients receiving conventional therapy - in some cases, greater. Clearly, we need to learn how to do better in the long-term management of lung and colorectal cancer - these cancers are notoriously resistant to chemotherapy - but even with these cancers, Oasis patients are doing considerably better than the average patient in the US. Note for example in lung cancer that chances of surviving for 2 years or more are strikingly higher at Oasis. The results in ovarian cancer are quite encouraging - at the 2-year point and beyond, chance of survival is about 3 times higher at Oasis. And note in particular the survival statistics for stage IV breast cancer patients who chose Oasis as their first therapeutic option - their chance of survival at 5 years is 75%, as compared with 20% in the US. These superior results in patients who came to Oasis of Hope first likely reflects the fact that these patients have not had previous chemotherapy, and therefore are more likely to respond to it than patients who have evolved resistance during previous therapy. The relative chemosensitivity of their cancers, in conjunction with the range of nutraceutical and drug adjuvants, that Oasis employs in hospital and in home care, is paying off greatly in long-term survival.
Table 2 summarizes 4-year survival in stage IV for breast (53 patients), lung (22 patients), and colorectal cancer (23 patients) in patients who have received the IRT-C protocol. As you can see, long-term survivals are about twice as high at any time point as compared with conventional US therapy - and considerably greater than that in the case of stage IV lung cancer. Ovarian cancer is not included in this analysis, because this type of cancer tends to be relatively chemosensitive, so we strongly advise the IRT-Q protocol for this cancer.
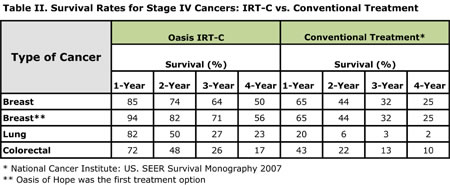
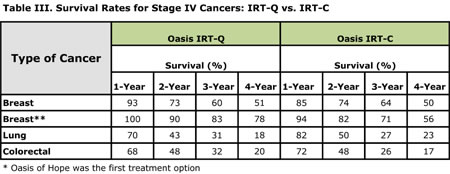
Table 3 compares the 4-year results in patients receiving IRT-Q or IRT-C at Oasis. Note that the long-term results of these protocols are not greatly different, with the exception of patients with stage IV breast cancer choosing Oasis as their first therapy option - they appear to do significantly better with the IRT-Q protocol, likely reflecting the fact that their cancers are prone to be chemosensitive when they come to Oasis of Hope.
Admittedly, we can't claim that many of these patients have been "cured" - in the sense that the cancer has been eliminated and won't come back. But it does seem that we are making some progress toward the goal of turning advanced cancer into a chronic disease that can be managed in the long term - rather like diabetes - as opposed to a rapid death sentence. And remember that our IRT protocols are in a constant state of evolution - barely a month goes by that we don't add some new element to our regimens, or modify them in a way that seems likely to improve their efficacy. In particular, our current statistics do not yet include patients who have received our new allogeneic lymphocyte immunotherapy, which was added to our IRT protocols about 2 years ago. So we are cautiously optimistic that we are on the right track, and that our results will continue to improve over the coming years.

Notes
1. Giunta R, Coppola A, Luongo C, et al. Ozonized autohemotransfusion improves hemorheological parameters and oxygen delivery to tissues in patients with peripheral occlusive arterial disease. Ann Hematol. 2001 December;80(12):745-748.
2. Clavo B, Perez JL, Lopez L, Suarez G, et al. Ozone therapy for tumor oxygenation: a pilot study. Evid Based Complement Alternat Med. 2004 June 1;1(1):93-98.
3. Bocci V, Larini A, Micheli V. Restoration of normoxia by ozone therapy may control neoplastic growth: a review and a working hypothesis. J Alternat Complement Med. 2005; 11(2):257-265.
4. Kwei KA, Finch JS, Thompson EJ, Bowden GT. Transcriptional repression of catalase in mouse skin tumor progression. Neoplasia. 2004 September;6(5):440-448.
5. Tas F, Hansel H, Belce A, et al. Oxidative stress in breast cancer. Med Oncol. 2005;22(1):11-15.
6. Vaquero EC, Edderkaoui M, Pandol SJ, Gukovsky I, Gukovskaya AS. Reactive oxygen species produced by NAD(P)H oxidase inhibit apoptosis in pancreatic cancer cells. J Biol Chem. 2004 August 13;279(33):34643-3454.
7. Lim SD, Sun C, Lambeth JD, et al. Increased Nox1 and hydrogen peroxide in prostate cancer. Prostate. 2005 Feb 1;62(2):200-207.
8. Chen Q, Espey MG, Krishna MC, et al. Pharmacologic ascorbic acid concentrations selectively kill cancer cells: action as a pro-drug to deliver hydrogen peroxide to tissues. Proc Natl Acad Sci USA. 2005 September 20;102(38):13604-13609.
9. Chen Q, Espey MG, Sun AY, et al. Ascorbate in pharmacologic concentrations selectively generates ascorbate radical and hydrogen peroxide in extracellular fluid in vivo. Proc Natl Acad Sci USA. 2007 May 22;104(21):8749-8754.
10.Padayatty SJ, Sun H, Wang Y, et al. Vitamin C pharmacokinetics: implications for oral and intravenous use. Ann Intern Med. 2004 April 6;140(7):533-537.
11.Padayatty SJ, Levine M. Reevaluation of ascorbate in cancer treatment: emerging evidence, open minds and serendipity. J Am Coll Nutr. 2000 August;19(4):423-425.
12.Riordan HD, Casciari JJ, Gonzalez MJ, et al. A pilot clinical study of continuous intravenous ascorbate in terminal cancer patients. P R Health Sci J. 2005 December;24(4):269-276.
13.Padayatty SJ, Riordan HD, Hewitt SM, Katz A, Hoffer LJ, Levine M. Intravenously administered vitamin C as cancer therapy: three cases. CMAJ. 2006 28;174(7):937-942.
14.Calderon PB, Cadrobbi J, Marques C, et al. Potential therapeutic application of the association of vitamins C and K3 in cancer treatment. Curr Med Chem. 2002;9(24):2271-2285.
15.Sharma RK, Marwaha N, Kumar P, Narang A. Effect of oral water soluble vitamin K on PIVKA-II levels in newborns. Indian Pediatr. 1995 August;32(8):863-867.
16.Zhang W, Negoro T, Satoh K, et al. Synergistic cytotoxic action of vitamin C and vitamin K3. Anticancer Res. 2001; 21(5):3439-3444.
17.Verrax J, Cadrobbi J, Delvaux M, et al. The association of vitamins C and K3 kills cancer cells mainly by autoschizis, a novel form of cell death. Basis for their potential use as coadjuvants in anticancer therapy. Eur J Med Chem. 2003 May;38(5):451-457.
18.De LW, Janssens J, Bonte J, Taper HS. Effects of sodium ascorbate (vitamin C) and 2-methyl-1,4-naphthoquinone (vitamin K3) treatment on human tumor cell growth in vitro. II. Synergism with combined chemotherapy action. Anticancer Res. 1993;13(1):103-106.
19.Kassouf W, Highshaw R, Nelkin GM, Dinney CP, Kamat AM. Vitamins C and K3 sensitize human urothelial tumors to gemcitabine. J Urol. 2006;176(4 Pt 1):1642-1647.
20.Tetef M, Margolin K, Ahn C, et al. Mitomycin C and menadione for the treatment of advanced gastrointestinal cancers: a phase II trial. J Cancer Res Clin Oncol. 1995;121(2):103-106.
21.Tetef M, Margolin K, Ahn C, et al. Mitomycin C and menadione for the treatment of lung cancer: a phase II trial. Invest New Drugs. 1995;13(2):157-162.
22.Alexandre J, Batteux F, Nicco C, et al. Accumulation of hydrogen peroxide is an early and crucial step for paclitaxel-induced cancer cell death both in vitro and in vivo. Int J Cancer. 2006 1;119(1):41-48.
23.Ramanathan B, Jan KY, Chen CH, et al. Resistance to paclitaxel is proportional to cellular total antioxidant capacity. Cancer Res. 2005; 15;65(18):8455-8460.
24.Chan MM, Soprano KJ, Weinstein K, Fong D. Epigallocatechin-3-gallate delivers hydrogen peroxide to induce death of ovarian cancer cells and enhances their cisplatin susceptibility. J Cell Physiol. 2006 May;207(2):389-396.
25.Teicher BA. Hypoxia and drug resistance. Cancer Metastasis Rev. 1994;13(2):139-168.
26.Kopp E, Ghosh S. Inhibition of NF-kappa B by sodium salicylate and aspirin. Science. 1994 August 12;265(5174):956-959.
27.Yin MJ, Yamamoto Y, Gaynor RB. The anti-inflammatory agents aspirin and salicylate inhibit the activity of I(kappa)B kinase-beta. Nature. 1998;396(6706):77-80.
28.Aggarwal BB. Nuclear factor-kappaB: the enemy within. Cancer Cell. 2004;6(3):203-208.
29.Cusack JC, Liu R, Baldwin AS. NF- kappa B and chemoresistance: potentiation of cancer drugs via inhibition of NF- kappa B. Drug Resist Updat. 1999;2(4):271-273.
30.Singh RP, Mallikarjuna GU, Sharma G, et al. Oral silibinin inhibits lung tumor growth in athymic nude mice and forms a novel chemocombination with doxorubicin targeting nuclear factor kappaB-mediated inducible chemoresistance. Clin Cancer Res. 2004;10(24):8641-8647.
31.Flaig TW, Su LJ, Harrison G, Agarwal R, Glode LM. Silibinin synergizes with mitoxantrone to inhibit cell growth and induce apoptosis in human prostate cancer cells. Int J Cancer. 2007 May 1;120(9):2028-2033.
32.Fakih M, Cao S, Durrani FA, Rustum YM. Selenium protects against toxicity induced by anticancer drugs and augments antitumor activity: a highly selective, new, and novel approach for the treatment of solid tumors. Clin Colorectal Cancer. 2005;5(2):132-135.
 Dr. Connealy graduated from the University of Texas School of Public Health and the University of Chicago Medical School. She then completed her postgraduate training at the Harbor/UCLA Medical Center in Los Angeles, California. A genuine health leader, Dr. Connealy has been published in the Journal of the American Nutraceutical Association (JANA), as well as in numerous health articles and magazines. She's also a frequent guest on TV and radio programs, and a guest speaker for professional organizations all over the country. Dr. Connealy is the editor of the Newport Natural Health Letter, a free weekly e-letter with insight that comes from more than 20 years of experience. Dr. Connealy is the founder and medical director of the Center for New Medicine in Orange County, California. The center focuses on the "root cause" of illness first, and treats everything from the common cold to cancer. To learn more, visit www.connealymd.com. Dr. Connealy graduated from the University of Texas School of Public Health and the University of Chicago Medical School. She then completed her postgraduate training at the Harbor/UCLA Medical Center in Los Angeles, California. A genuine health leader, Dr. Connealy has been published in the Journal of the American Nutraceutical Association (JANA), as well as in numerous health articles and magazines. She's also a frequent guest on TV and radio programs, and a guest speaker for professional organizations all over the country. Dr. Connealy is the editor of the Newport Natural Health Letter, a free weekly e-letter with insight that comes from more than 20 years of experience. Dr. Connealy is the founder and medical director of the Center for New Medicine in Orange County, California. The center focuses on the "root cause" of illness first, and treats everything from the common cold to cancer. To learn more, visit www.connealymd.com.
Francisco Contreras, MD, completed medical school at the Universidad Autonoma de Mexico in 1978. He joined his father, world-renowned Ernesto Contreras, MD, at Oasis of Hope Hospital in 1983. In 2009, Dr. Contreras provided Dr. Connealy licensing rights to open an outpatient clinic in Irvine, California, as he admired her work with cancer patients. To learn more visit www.oasisofhopeusa.com.
|



