Author's
Note: "Down's syndrome" was a term formerly used
to describe these patients, but that is no longer the proper terminology.
The use of People First Terminology is important when working with
these patients and their families and advocates. People First Terminology
encourages us to refer to the person first and the disability second.
The Down syndrome does not define these children or adults. It is not
their identity. It is only one thing about them. So we do not say "a
Down syndrome child." We say "a child with Down syndrome" today.

Page 1, 2, References
 I have been very fortunate this year
to work with 15 families whose children have Down syndrome. This
essay will describe these children's' histories,
their clinical findings, and their evaluation and treatment using applied
kinesiology methods. I have been very fortunate this year
to work with 15 families whose children have Down syndrome. This
essay will describe these children's' histories,
their clinical findings, and their evaluation and treatment using applied
kinesiology methods.
People with mental and physical disabilities are the largest minority
group in this country. They outnumber Latinos, African-Americans, and
Asians. People with Down syndrome are now living at home within our
communities. They are growing up with their peers at school and at
play, working side by side, dating and living independently, and growing
old. Their lives now present new opportunities and challenges to conquer
for themselves and for those who work and live with them every day.
People with physical and mental disabilities are going to be seen,
increasingly, as the individuals they are, with individual abilities
that are going to be nurtured and enhanced. I think we are going to
recognize that they have individual personalities to be appreciated,
individual lifestyles to be lived fully and with gusto, just like everybody
else. And, frankly, with our gifts in the evaluation and treatment
of neurologic disorders, chiropractic and other holistic physicians
with skills in the cranial arts should be on the front lines of the
coming renaissance for these people. If you can make contact with a
few of these patients or their advocates in your community and increase
their level of health by your service, you will open a doorway that
will increase your reputation and your practice in your community.
Introduction
There is evidence in ancient art and literature that people with trisomy 21
have long been part of the human race. In 1866, Dr. John Langdon Down first
remarked on the facial similarities of a group of his mentally retarded patients.
With the identification of the chromosomal basis of Down syndrome in 1959,
a gradual process of acceptance of trisomy 21 as being a variation of normal
began to remove some of the handicap and end the uninformed debates over
the "humanity" of people with Down syndrome. Down syndrome is
the most common readily identifiable cause of intellectual disability, accounting
for almost one-third of all cases. It occurs equally in all races with an
overall incidence of approximately one in 800 births; approximately 4,000
children with Down syndrome are born each year. This is much lower than the
actual conception rate due to a high incidence of spontaneous and surgical
abortion. Congenital heart disease affects 40% of these babies. Severe congenital
heart disease remains a major killer of children with Down syndrome, despite
advances in surgical treatment. In the absence of a congenital heart defect,
the majority of children can expect to live into their sixth decade. Up to
15% of children with Down syndrome will have radiological evidence of instability
of the atlantoaxial joint, but in only a handful of cases will this instability
result in an impingement of the spinal cord with resultant neurological signs.
Many reasons have been proposed in the literature about the causes of the
improper cell division that leads to Down syndrome (Trisomy 21); genetic
predisposition, maternal age, hormonal abnormalities, X-ray exposure, immunologic
problems, potent drugs, and viral infection may be involved in these patients' history.
People with Down syndrome now compete in the nation's work force. They
used to live in segregated day programs of which there are, even today, over
7,000 in the US. Real work is now commonplace for these patients. This is a
program called "supported employment." The basic notion involves
the use of a trained staff person who accompanies the person with a disability
into a paid placement in the workplace. Between 1985 and 1995, there was growth
of this program from less than 10,000 people with disabilities in supported
employment to over 150,000.
Children with Down syndrome will be developmentally slower than their siblings
and peers and have intellectual functioning in the moderately disabled range,
but the range is enormous, and the distance from their peers is the crucial
factor where chiropractic and cranial therapeutics can make a profound difference.
Neuromusculoskeletal Disorders in Down Syndrome
The cranial structure of the child with Down syndrome presents certain variations
from the normal anatomic pattern that result in the characteristic slanting
eyes, undeveloped nasion, infantile features, and so on. In children with
Down syndrome, the head has been described as brachycephalic, which is a
shortening of the anteroposterior diameter with flattening of the occiput.
Brachycephalic heads produce an anterior displacement of the condylar parts
of the occiput into the facets of the atlas. The posterior arch of the atlas
vertebra may also approximate the odontoid process of the axis. The vertebral
canal may be narrowed, with possible impingement of the medulla and increasing
tensions upon the craniosacral reciprocal tension membranes (RTM). This one
primary cranial distortion produces profound consequences throughout the
spine and pelvis. Usually the heads of children with Down syndrome are smaller
than in age-equivalent children who do not have Down syndrome; thus, the
cranial capacity is reduced. The nasal bones are poorly developed, and the
maxilla as well as the sphenoid has been described as hypoplastic. Frequently,
the palate is narrow and short, which, together with the maxillary hypoplasia,
results in a small oral cavity. These features may be improved with proper
cranial therapy.
It has been postulated that children with Down syndrome have an intrinsic defect
of their connective tissue that is responsible for the observed general ligamentous
laxity. Recently, it has been shown that fetal heart collagen is encoded by
two genes mapped on the distal part of the long arm of chromosome 21.1 There
are specific musculoskeletal disorders such as atlantoaxial instability, hip
dislocation, patellar subluxation, and others that deserve special attention.
The pelvic bones of infants with Down syndrome usually show flattening of the
acetabular angle, widening of the iliac wings, small ischial rami, and coxa
valga of the femur.
However, because muscle tone and neurological disorganization can be corrected
so quickly using proper cranial and other natural health care procedures, the
question of whether these genetic disorders are the cause of these problems
should be investigated in every patient.
In most of these cases of Down syndrome, I found that the occiput was deformed
to a greater or lesser degree. This interosseous cranial fault of the occiput,
called the universal cranial fault in applied kinesiology, has been described
by Drs. Goodheart, Walther, DeJarnette, Sutherland, Magoun, Arbuckle, Frymann,
Upledger, and many others. (See Figure 1.) The amount of this deformity has
shown some correlation with the extent and severity of the disabilities in
the child.2-9
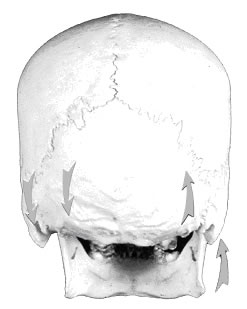 Figure 1: The Occiput and Cerebellum in
Down Syndrome Figure 1: The Occiput and Cerebellum in
Down Syndrome
The interosseous distortion of the occiput (the universal Cranial Fault)
changes the position of the condyles, the shape of the foramen magnum,
the position and shape of the jugular foramina, the elasticity of the
tentorium, the drainage of blood from the head, the movement of cerebral
spinal fluid (CSF) through the interstices of the brain, the shape
of the cerebellum itself, and increases the tension upon the cranial
membranes throughout the skull. This distortion is transmitted to all
the other bones of the skull. *
The growth of the brain is definitely affected by the resistance it meets.
As the skeleton and muscles give the body its shape, so do the cranium and
dura help maintain the shape of the brain as it checks, guides, and coordinates
the brain's movement. With many children who have extensive cranial structural
anomalies and faults, it would not be possible for either the cerebellum or
the frontal lobes to grow symmetrically without proper cranial corrections.
Flattening of the occiput on one or both sides was a common finding in these
patients (approximately 90%). The head was shortened in its anteroposterior
diameter and very wide transversely. The lateral angles of the flattened occiput
produce a spreading pressure upon the parietal bones. The petrous portions
of the temporals was also put into external rotation, thus putting extra tension
on the tentorium and pulling the falx down. Whenever we see a flattened occiput
in a patient, it is vital that we evaluate for cerebellar disturbances.
Confusion of the basilar bones as a result of the flattened occiput produces
abnormal tensions in the membranes that may cause crowding of the cerebellum
low in the posterior cranial fossa, forcing the medulla and pyramidal tracts
against the basilar portion of the occiput. (See Figure
2.) If the medulla
and motor tracts of the cord as they leave the medulla have been forced low
in the posterior cranial fossa against the rim of the foramen magnum, imagine
then what kind of additional tensions will be created for the little child
with a subluxation of the atlas vertebra.
Figure
2: Cranial Base Superior View 
Almost
every major nerve pathway from the brain to the body and from the body
to the brain pass through the space contained within
the
developing portions
of the occiput. Besides the effect of the pressure of this crowding upon
the cerebellum and brainstem, and cranial nerves 9-12,
there will also be dramatic changes in the spaces through which
cerebrospinal fluid must pass.
This is where the hypoglossal nerve to the tongue and the vagus nerve to
the digestive tract pass out through the skull. These are the areas that
are the
first to show the stress of birth (vomiting, an inability to suckle, spitting
up). Deformities of this area of the skull were very common in the children
with Down syndrome I have treated, and the injury to the nervous system
found there varied from the child who had mild spitting-up difficulties
to the child
who was very passive to the child who was hyperactive, aggressive, with
behavior problems, and so on. This is a very critical area, one that we
should always
evaluate when we treat newborn babies.
The junction of the medulla oblongata and the spinal cord at the level
of the occipito-atlantal articulation is crucial to normalize in these
patients.
The
pyramidal tracts above this level and the decussation of the pyramidal
tracts just below rest upon the basilar portion of the occiput. The
extra pyramidal
tracts situated laterally at this level are involved with muscle tone.
Hypotonia (the "floppy baby" phenomenon, which is a very
common finding in children with Down syndrome) may be the manifestation
of dysfunctions
at
this level.
The occiput originates from four parts at birth, and these are not fully
united into a single bone until the child is around six years of age. Because
these
multiplicities of articulations are held in place primarily by the membranous
tensions in the meninges, it is imperative that we correct cranial faults
as early in life as possible. Any interosseous distortions that remain
in a child
after the age of six are much more difficult to correct. The consequences
of leaving them uncorrected may be the difference between normal and abnormal
development of the entire central nervous system. Any of the twenty-four
cranial
nerves can be affected by interosseous distortions of the cranium.
The four developing parts of the occiput circle the large hole of the foramen
magnum, through which the brain stem passes. When the occiput is flat or
its squama, condylar, or basilar portions are warped (posterior on one
side and
anterior on the other), you can assume that the foramen magnum will not
be symmetrical, and that it is narrowed on one side compared to the other.
Applied
Kinesiology challenge procedures to the condylar portions of the occiput
can determine this.
The strain created within the cranium by the universal cranial fault is
transferred to the central joint of the skull, between the sphenoid and
the occiput, called
the sphenobasilar joint. The tension placed upon the pyramidal tracts,
the medulla, and the cranial nerves at the base of the skull can be imagined
if
you visualize the sphenobasilar articulation from above. If there is a
turning, twisting, or side-bending of this joint, and if the joint is additionally
in
flexion or extension, as is so often the case, then the added strain on
the overlying pyramidal tracts, medulla, cranial nerve foramina, and the
cerebral
aqueducts should be apparent. (See Figure 3.)
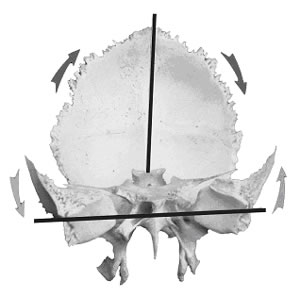
Figure 3:
The Universal Cranial Fault
The universal cranial fault produces counter-rotation of the sphenoid
and occipital bones. The sphenoid is the most complex bone in the
body. Twelve of the twenty-four cranial nerves pass through or over
it. The pituitary gland is cinched into the sphenoid by the roof
of the tentorium cerebelli. The sphenoid has extensive muscular attachments
to the temporomandibular joint. Because of the interleaving of the
reciprocal tension membranes, any fault of the sphenoid will create
tensions throughout the cranial mechanism, and vice versa.
The slanting eyes commonly found in children with Down syndrome are
a developmental distortion of the sphenoid. (See Figure 4.)
The myopia or cross-eyes are due to the same distortion, thereby displacing
the origins of the extrinsic muscles
of the eyeball around the optic foramen in the roots of the lesser wing
of the sphenoid.
Figure 4: Sphenoid
Bone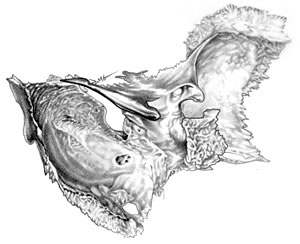
Another
factor relating to the growth potentials in children with Down syndrome
may be the pituitary gland, whose neural, endocrine,
vascular,
and cerebrospinal
fluid components are modified by the dural investments, which cinch
it into place from at least four directions laterally, and from above
and
below as
well.
The dura, the diaphragma sella, the falx, and the tentorium all bring
the pituitary into a fundamental mechanical relationship with the sphenobasilar
joint (synchon-drosis).
Any tilting of the sphenoid (producing the slightly slanted eyes in
children with Down syndrome) will be transmitted to the diaphragma
sella, attached
to the clinoid processes, and blended with the contiguous and surrounding
dura
mater. (See Figure 5.) This tension may
be transmitted to the infundibulum, which connects the pituitary to
the hypothalamus.
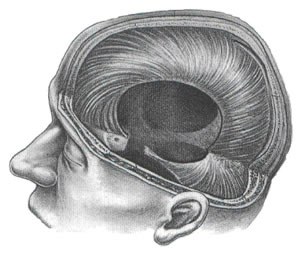 Figure 5: Cranial System Figure 5: Cranial System
Eighty percent of the nervous system operates within the mobile compartments
shown below. Hundreds of research studies have now demonstrated the
movement potentials and neurological consequences of immobility in
the cranial system.10 Dural tension anywhere in the cranial-sacral
system can be transmitted to the pituitary gland and hypothalamus
and may affect growth or endocrine function. Cranial tissue tension
and organ function is thereby mechanically related to cranial respiratory
function.
According to Best and Taylor, 100,000 fibers pass through the infundibulum.
The shape of the sphenoid and the position of the sphenobasilar synchondrosis
will influence the position of, and the tension upon, the foramen
in the diaphragma sella through which the infundibulum passes. This
mechanical
fault at the center
of the autonomic and endocrine systems is crucial to normalize if
possible. Insistent and prolonged molding of the cranial base and
freeing of
the sutures to stimulate pituitary action can be of considerable
significance in these
cases. Case 9 below demonstrates this phenomenon.
Applied Kinesiology Chiropractic: A Profile
Applied Kinesiology (AK) is a method of chiropractic founded by George J. Goodheart,
Jr., a chiropractic physician practicing near Detroit, Michigan. AK has been
in the chiropractic profession for over 42 years and is now used throughout
the healing professions. In a survey by the National Board of Chiropractic
Examiners in 2000, 43.2% of respondents stated that they used AK in their
practices, up from 37.2% of respondents who reported they used AK in 1991,11-13
with similar numbers reported in Australia.14 The general public's
awareness of manual muscle testing (MMT) and AK has also been increased worldwide
by virtue of the patient education program Touch for Health (T4H), designed
by an International College of Applied Kinesiology (ICAK) diplomate, John
Thie. T4H was one of the first public self-help programs and is the fastest
growing "body work" program in the world, used by over ten million
people. The Touch for Health book is the largest selling complementary health
book in the world, with 12 million copies sold in over 40 countries.15
AK employs manual muscle testing (MMT) as a major part of evaluating patients
in conjunction with standard natural health care evaluations and diagnostic
modalities. Successive diagnostic and therapeutic procedures were developed
for the objective testing (MMT) of neurolymphatic reflexes, neurovascular reflexes,
and cerebrospinal fluid flow, from ideas originally described by Frank Chapman,
DO, Terrance J. Bennett, DC, and William G. Sutherland, DO, respectively. Later,
influenced by the writings of Felix Mann, MD, Goodheart incorporated acupuncture
meridian therapy into the AK system. Additionally, the vertebral challenge
method (1972) and therapy localization technique (1974) were added. The correlation
of nutritional influences on muscle physiology has also been extensively studied.
The myofascial ideas of Fulford, Jones, and Travell are also an important part
of the AK system.16 The work of Major B. DeJarnette, DO, DC, and founder of
the sacro-occipital technique (SOT), is also a major part of AK's diagnostic
and therapeutic procedures.4
During an AK examination, the doctor looks for patterns of inhibition (weakness)
and facilitation (strength) in the nervous system. MMT evaluates the anterior
horn motor neurons to a muscle, and a treatment that improves the facilitation
(strength) of a muscle also improves the function on the final common pathway
to muscles in the anterior horn motor neurons of the spinal cord, as well as
the motor portion of the cranial nerves. Because of the communication systems
in the body between the nervous, circulatory, and muscular tissues, a disturbed
portion of the muscular system can impair the function of other tissues and
organs, especially those with which it is neurologically and anatomically most
closely related. The overall tone of the nervous system is thought to be evaluated
and treated using these methods. Since 1964, the AK community of physicians
worldwide (members of the International College of Applied Kinesiology) has
continued to test various therapeutic approaches using manual muscle testing
as a clinical parameter for the measurement of physiologic response and the
restoration of normal muscle function.
AK is a novel diagnostic and therapeutic chiropractic technique that has support
within the chiropractic, dental, biofeedback, acupuncture, veterinary, and
other health care modalities. Even with the wide popularity that MMT has achieved
among chiropractors and other physicians in the United States and around the
world, few practitioners are familiar with the laboratory research underlying
AK MMT procedures.17-65 AK uses a method of diagnosis with specific methods
of MMT to guide treatment and to validate the effectiveness of care rendered
to the patient.
As with most chiropractic techniques, the research is ongoing and in the developmental
phase, however, there is mounting evidence of its clinical effectiveness and
greater studies are warranted.66-68 Hopefully this paper has stimulated the
desire to review the current AK literature and become an effective user of
and contributor to chiropractic AK research.69-71
It is very difficult to localize and distinguish between the various palpated
and tested tissues in the cranial area. Only by having a thorough knowledge
of both the external and internal anatomy of the skull can this be accomplished.
However the internal cranial tissues can be specifically tested using non-invasive
AK MMT procedures, and the muscle changes found can be anatomically interpreted
by the physician as to the location of the primary involvement: cranial bone
involved, foraminal and cranial nerve entrapment suspected, extra-cranial muscular
involvement, and so on.2-3 Specific cranial and vertebral challenges and MMT
offers us the best way to differentially diagnose a cranial bone problem from
many other problems in this wonderfully complex area. Using MMT, a physician
can make rapid, accurate, and highly specific assessments of the cranio-sacral
mechanism. Adding this mode of evaluation and treatment to your daily patient
visits should expand your scope of practice and your reputation among your
patients.
Page 1, 2, References
|



