|
Full version online
Page 1, 2, 3, 4
Abstract
Introduction: The correlations between salivary hormone testing and the manual muscle test have not to our knowledge been reported before. Methods: Correlations between manual muscle tests and salivary hormone tests for 110 participants (83 female, 17 male) experiencing adrenal stress disorder (ASD) are described. Saliva samples were collected and screened for cortisol and dehydroepiandrosterone (DHEA). Results: We observed that patients with signs and symptoms of ASD and abnormal hormone levels on salivary hormone testing demonstrate distinct neuromuscular impairments that could be detected using the MMT. Discussion: Evidence for the linkages between neurohormonal imbalances and muscular imbalances are presented. Conclusion: This physical examination procedure, used within a number of health professions, may warrant further investigation given its utility, noninvasiveness, rapidity, and cost-effectiveness as a day-to-day clinical evaluation and management tool in cases of ASD.

Introduction:
Adrenal Stress Disorder, Clinical Prediction Rules, and the Manual Muscle Test
Adrenal gland imbalances are one of the most common conditions in the world, and stress-related illnesses are one of the most common conditions faced by functional medical physicians.1,2 Serum blood samples and salivary hormone testing are standard diagnostic procedures for patients with "stress-related illnesses"; however, these diagnostic procedures cannot be performed on every patient who may be experiencing adrenal stress disorder (ASD), nor can it affordably be performed repeatedly on established patients or in patients who are undergoing recovery from this condition, due to their cost.3,4 In these patients with chronic stress, new stressors often arise and repeating the salivary hormone test during the course of a lifetime becomes more and more unwieldy. Additionally, a single serum blood sample or salivary hormone test for ASD is insufficient for treatment; a second and even a third must be performed to determine whether the treatment protocol being used is working.5
However, previous research has shown the advantage of salivary cortisol measurements over serum measurements in the management of patients with ASD.6 The advantages (simplicity, decreased stress during the procedure, convenience, sample mail-in and temperature stability) have been described, and for these reasons this method was chosen in order to compare the physical applied kinesiology manual muscle test (AK MMT) examination with this laboratory test.7,8
Clinical prediction rules (CPRs) are derived statistically from research evidence with the aim of identifying the combinations of clinical examination findings that can predict a condition or outcome or favorable response.9–11
CPRs quantify the contribution of symptoms, clinical signs, and available diagnostic tests, and stratify patients according to the probability of having a target disorder. The outcome of interest can be diverse and be anywhere along the diagnostic, prognostic, and therapeutic spectrum.12
Essentially, the identification of responder subgroups is now a treatment priority, because it appears that larger treatment effects are observed if focused nutritional therapy is applied to those likely to respond.13
In a typical biomedical and complementary and alternative medical clinical encounter, a patient seeks care due to stress-related illness or neuromusculoskeletal pain. The doctor performs a battery of tests that detects their chemical imbalance or reproduces the patient's pain; accordingly, the patient is deemed to have stress-related hormone imbalance or neuromusculoskeletal pain. This is a somewhat circular process. Simply to give a label to a patient that summarizes what was acquired by way of testing is not an ideal form of diagnosis.
When diagnostic methods have a capacity to specify the form of therapy needed, or if they can provide the prognosis or long-term course of a disorder, they have more value. Salivary (or serum blood) testing may help guide physicians to the hormonal imbalances present in a patient with ASD, but it will not tell them how to best treat the problem. As an alternative, the manual muscle test identifies a functional disorder (inhibition) of the locomotor system. In the applied kinesiology (AK) evaluation of cases of adrenal stress disorder (ASD), this muscle inhibition occurs in specific muscles that immediately respond to specific adrenal gland nutritional support and/or adrenal gland viscerosomatic reflex stimulation (therapy localization).14
For example, a patient with a low DHEA value may need the actual hormone DHEA or may show a need for a vitamin or mineral supplement that acts as a substrate to synthesize DHEA in order to strengthen the inhibited adrenal-related muscle. The physical examination procedure presented here provides information about the patient with "stress-related illness" that we did not previously know. This functional disorder associated with the adrenal-stress patient (the attendant viscerosomatic muscle inhibition) removes circularity from the AK method of diagnosis; the treatment required to remove this diagnostic finding in the adrenal-stress patient is what immediately strengthens the muscular inhibition. The corrective approach is thereby contained within the diagnostic procedure.
AK practice and experience has shown that, when a substance comes into contact with the tongue, there is an immediate change in muscle function as determined by the manual muscle test.15,16 It seems evident that the effect is due to stimulation of the gustatory and olfactory receptors.17 Certain substances enter the bloodstream almost immediately by oral absorption, such as sodium and sugar. For instance, patients with untreated Addison's disease have increased taste sensitivity, roughly 100 times more acute than that of normal participants.18 In the case of sugar, considerable neurophysiologic action appears to take place from sugar stimulation to the gustatory receptors. For instance many diabetics carry sugar products to combat hypoglycemia and malaise as a result of excessive insulin administration. Within about twenty seconds after putting the sugar product in their mouth, they feel better. The effect is preabsorptive. It cannot take place from absorption into the bloodstream because of the short time factor and the small amount of sugar product ingested.19
Several cardiac medications are administered sublingually. Cardiac muscle function changes within 10 minutes of the sublingual administration of molsidomine, as indicated by ECG.20 There is an improved absorption of tetranitrate (a medication for angina pectoris) sublingually as opposed to the buccal pouch. It is effective when administered buccally, topically, or injection; it is considerably less effective when merely swallowed.21
Because muscle dysfunction frequently reflects biochemical dysfunction, the use of the AK MMT may expedite the broad-scope discovery of the causes of biochemical disorders.22,23 Goodheart originally observed, "The opportunity to use the body as an instrument of laboratory analysis is unparalleled in modern therapy; if one approaches the problem correctly, making the proper and adequate diagnosis and treatment, the response is satisfactory to both the doctor and the patient."24 If it proves to be the case that the AK MMT is sensitive and selective to ASD, then the factors that correct the muscle inhibitions found to be related to the adrenal gland may become an important guide in the selection of treatment modalities and nutritional elements in these cases.
Chewing the substance is the most effective means of testing because it simulates the oral movements of eating. There is an increased response from the oral chemoreceptors if the papillae are moved in conjunction with the substance tested.17 The testing of nutrition as advocated by the International College of Applied Kinesiology is a discipline limited to the tested substance stimulating the gustatory or olfactory nerve receptors, combined with accurate and specific muscle testing.25
The MMT diagnosis of inhibited muscles and their covariance with patients' biochemical dysfunctions tells us something about the status of their condition as well as the responsiveness of this biochemical disorder to nutritional treatment.14,16,26–28 The immediate improvement in muscle strength (associated with patients' biochemical dysfunctions) that occurs after ingestion of the appropriate nutrient(s) that has been reported clinically, suggests this correlation as well.29
Our approach in this case series has been to determine the concurrent validity of the AK MMT diagnostic method compared to an established, "gold standard" biochemical testing method, the salivary hormone test. The usual form for evaluating the concurrent validity of a test is to check any newly developed method of diagnosis against a method which has long been identified as a useful measure or reliable method of diagnosis. Were the AK sensorimotor tests of the biochemical component of ASD consistent with the findings of this laboratory test?
But why would we want to evaluate salivary hormone levels using something other than what has been regarded as the "gold standard" tests? In the daily treatment of patients, using salivary hormone testing on an on-going, repeated basis is both time-consuming and expensive. In the management of a patient with ASD, an immediate, inexpensive evaluation tool of their adrenal glands' status would be desirable.
Methods
One hundred and ten participants were selected over a 2-year period from patients presenting at three participating clinics, in Pueblo, Colorado (US); Chapel Hill, North Carolina (US); and Melbourne (Australia). The clinicians each had over 10 years of experience using the AK MMT. Being able to employ the AK MMT in a manner whose inter- and intraexaminer reliability and construct, concurrent, and predictive validity have all been documented requires considerable training on the part of the examiner.30 Caruso and Leisman showed that examiners using the MMT with 5 years' experience have virtually perfect correlation with objective measurements by instrumentation for over 700 muscle tests.31
Participants were 83 female and 17 male patients between ages 13 and 72 (average age 41.4 years), who met the following inclusion criteria: experiencing self-reported "stress" symptoms and willing and able to undergo both AK chiropractic physical examination and salivary hormone testing (for which the patient paid approximately $300 US). Participants were not included in this study if they had any contraindications to chiropractic treatment, or if they were currently on any steroid or hormone medication. Participants were then briefed on the AK method of diagnosis and treatment, and the possible benefits and risks of treatment. Both verbal and written informed consent was obtained before assessment and treatment began.
For each participant in this case-series report, the focus was upon the Adrenal Salivary Index (ASI). The ASI offers the clinician and the patient an evaluation of the cortisol levels at various times of the day and a reading of the DHEA levels. It also offers a rating of overall adrenal function from normal to failure. A number of research studies have validated saliva as a diagnostic medium to measure the unbound, biologically active fraction of steroid hormones in the bloodstream. Saliva is a natural ultrafiltrate of blood, and steroids not bound by carrier proteins in the blood freely diffuse into saliva.
Intervention
The protocol in this study was as follows:
- A complete patient history was taken.
- In the initial examination, each patient's blood pressure was tested in three positions (supine, seated, then standing), in addition to pupillary reflexes, Rogoff's sign, heart sounds, and ligament stretch reaction. (These physical tests are additional physical signs in AK examination regimen of adrenal gland dysfunctions.)32
- The patient was physically examined with the focus upon the symptom history, particularly upon the function of muscles and joints and reflexes related in applied kinesiology to the adrenal gland (Figure 1).
- These muscles are the sartorius, gracilis, or posterior tibialis (Figures 2–4).26
- If these muscles were initially strong, then the sensorimotor stimulation (therapy localization in AK) of the adrenal glands' viscerosomatic reflexes (i.e. Chapman's and Bennett's and acupuncture meridian points) was implemented during the MMT (Figures 1, 5–7).14,26,33 If change in strength of the muscle occurred, this was noted (Table 1).
- After the assessment, the participant was given verbal and written instructions on how to perform the salivary hormone test correctly. The participant took the test kit home and collected saliva samples in collection tubes in the morning, at noon, in the afternoon, and at bedtime. These were placed in a plastic, resealable bag and immediately sent to the laboratory via the postal service. The hormones evaluated by the laboratories in this study were cortisol (diurnal, 4 times daily), and DHEA. These saliva tests used an enzyme-immunoassay, but to solve the problem of the matrix effect for hormones at very low concentrations in saliva, an extraction step was used. This removed the contaminants that may interfere with the assay and yielded results comparable with those seen in published studies where highly sensitive assays have been used.34
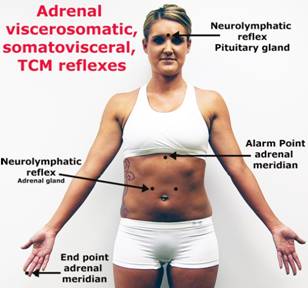 |
Figure 1: Viscerosomatic reflexes related to the adrenal glands. Participants touch these specific areas while the MMT is performed; if immediate muscle strength changes result, it is considered a positive test.
|
Page 1, 2, 3, 4
|




