|
Introduction
The iodine loading test was introduced in 2004 by Abraham et al. to determine iodine levels in urine after a supplemental dose of an iodine/iodide mixture.1 The test is based on the theory that following oral consumption of 50 mg iodine/iodide, all iodine not excreted within a 24-hour period is retained and utilized by the body.2,3 An arbitrary cutoff of 90% excretion of the 50 mg iodine/iodide dose during the 24-hour testing period is used to determine whether a patient has reached whole body iodine sufficiency.4 People undergoing the test are deemed to be deficient in iodine if they excrete less than 90% of the iodine loading dose.3,5,6 It is well documented that over 90% of a nutritional dose of iodine (such as several hundred micrograms) is excreted in urine, but not necessarily within the first 24 hours after ingestion.7
One advocate of the iodine loading test reported that 96.5% of over 4000 patients they tested were iodine deficient.5 Similarly, another advocate found that of 4065 patients tested, less than 1% excreted more than 90% of the 50 mg iodine/iodide loading dose.6 Both studies indicate an extremely high rate of iodine insufficiency in tested subjects. In comparison, de Benoist et al. report that 89% of the general American population have sufficient iodine intake based on the World Health Organization Global Database on Iodine Deficiency.8 This significant discrepancy has created confusion in the medical world over who is at risk of iodine deficiency disorders and the difference between iodine sufficiency/deficiency and whole-body iodine sufficiency/deficiency.
Our goal in this study was to analyze urine iodine excretion kinetics before and after a 50 mg iodine/iodide loading dose and to investigate the arbitrary iodine loading test cutoff of 90% excretion used to determine whole-body iodine sufficiency.
Materials and Methods
Ten volunteers from ZRT Laboratory, five men and five women with no history of iodine supplementation, participated in the study. Each participant was provided with four 24-hour collection vessels, an unlimited supply of 5 mL polypropylene tubes, and four 12.5 mg Iodoral (5 mg iodine and 7.5 mg iodide) tablets (Optimox Corporation; Torrance, CA). Participants were instructed to complete four subsequent 24-hour collections, including collections of each individual urine void. Twenty-four hour collections began with the second urine void of the day and ended with the first urine void the following morning. A 4 mL aliquot of each individual urine void was stored in a polypropylene tube before the remainder of the void was collected in the 24-hour container. After completion of the first 24-hour collection to establish baseline urine iodine levels, four tablets of Iodoral containing a total of 50 mg of iodine/iodide were immediately consumed. The final three 24-hour collections were completed without any further iodine supplementation.
Urine samples were assayed for iodine according to the method described by Ohashi et al. and for creatinine using Jaffe's reaction.9,10 One female participant had an incomplete collection and was excluded from the study. Iodoral dissolved in synthetic urine (Surine; DTI Innovative Products), ICP-MS determined EQUIP samples (Ensuring the Quality of Iodine Procedures; Centers for Disease Control), and Seronorm urine (Seronorm Trace Elements; Sero AS, Norway) were used as controls. Total urine iodine was determined in the 24-hour samples by multiplying the iodine result in µg/L by the liters of urine in the corresponding 24-hour sample. Individual urine samples were corrected with creatinine to adjust for hydration status, and reported as µg iodine/g creatinine by dividing the iodine result in µg/L by the creatinine result in mg/mL.
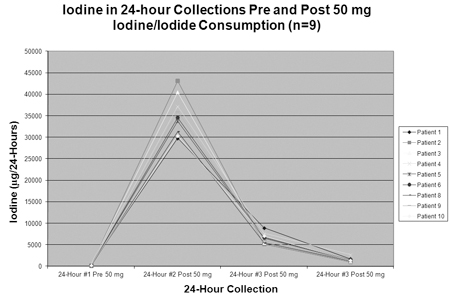
Figure 1
Results
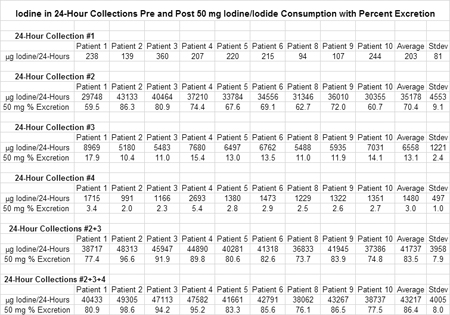
Twenty-four hour iodine excretions varied between individuals both before and after consumption of 50 mg iodine/iodide, but excretion kinetics were similar in all participants (Figure 1). The average amounts of iodine detected in the first, second, third, and fourth 24-hour collections were 203, 35178, 6558, and 1480 µg/24-hours with standard deviations of 81, 4553, 1221, and 497 µg/24-hours, respectively (Table 1). During the first 24-hour period following consumption of 50 mg iodine/iodide, an average of 35178 µg iodine (35.2 mg) was excreted by study participants, accounting for 70.4% of the loading dose. Average iodine excretions of 6558 µg (6.6 mg) and 1480 µg (1.4 mg) in the third and fourth 24-hour collections following the standard 24-hour loading period accounted for 16.1% of the 50 mg iodine/iodide dose.
Table 1 (Larger 1.14MB image here)
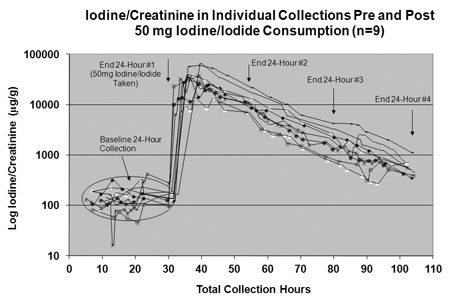
Excretion of iodine in individual urine voids collected over a 96-hour period, before and after ingestion of the 50 mg iodine/iodine dose, are shown in Figure 2. Results are shown on a log scale because of the exponential drop in iodine levels following the initial peak after ingestion.
Figure 2
Discussion
We aimed to study iodine excretion before and after consumption of a 50 mg dose of iodine/iodide and determine whether it was reasonable to expect 90% of the dose to be excreted within the first 24 hours after ingestion. Our data show that significant iodine excretion continues after the standard 24-hour duration of the iodine loading test, with an average of 16.1% of the 50 mg iodine/iodide loading dose excreted during the final 48-hour period of our study. With such a large amount of iodine excreted after the standard 24-hour loading period, it is reasonable to assume that 90% or greater excretion of a 50 mg iodine/iodide loading dose is difficult, if not impossible, to achieve.
Proponents of the iodine loading test recommend that testing be repeated 3 months after supplementation with 12.5 to 50 mg iodine/iodide per day to reassess the iodine status of the whole body.13 However, if iodine supplementation is not discontinued for several days before testing, residual supplemental iodine will be excreted along with the 50 mg loading dose, giving a test result showing a false high excretion. Abraham et al. recommend discontinuing iodine supplementation only 24 to 48 hours before the loading test, which would be insufficient time to clear the previous iodine supplementation, as shown in our study.14 Patients undergoing a loading test such a short time after stopping prior supplementation might falsely conclude from their loading test excretion results that their habitual high dose iodine supplementation has increased their total body iodine saturation.
Based on iodine loading test results, Abraham estimates that the amount of iodine that can accumulate in the body can reach over 1500 mg once whole body iodine sufficiency is reached.2 The author's assumption is that the iodine not excreted during the loading test is being held on to and utilized by the body. This might be true if iodine excretion following a 50 mg dose of iodine/iodide only occurred during the 24-hour period of the loading test, which is not the case. Furthermore, iodine is also excreted in feces and sweat, neither of which are accounted for when testing urine.11,12 Iodine excretion in feces could easily be tested to determine the percentage of the 50 mg iodine/iodine loading dose not absorbed by the gastrointestinal tract. Without data on how much iodine is being absorbed, it is impossible to estimate how much, if any, of the iodine that is not excreted in the urine is actually accumulating in the body. A reevaluation of the total amount of iodine retained by the body once it reaches whole body iodine sufficiency is necessary.
In general, a 24-hour collection poses multiple problems, both for the patient and the outcome of the loading test. Missed urine collections and incomplete urine catches during bowel movements can cause significant iodine losses depending on when they occur. A complete collection is needed to accurately determine how much of a 50 mg dose of iodine/iodide is excreted in the urine. Studies have shown that 10% to 20% of 24-hour collections are inappropriately collected or incomplete.15-17Any urine loss during the 24-hour loading test could result in a lower percent excretion and a failed iodine loading test.
In conclusion, modifications need be made to the iodine loading test before it is used to determine whole body iodine sufficiency or a need for supplemental iodine. Currently the iodine loading test does not provide a realistic assessment of an individual's whole body iodine sufficiency or deficiency due to flaws in the methodology and the use of an arbitrary excretion cutoff point. Extending the iodine loading test's collection period past 24 hours and including analysis of iodine in feces would provide a better picture of iodine retention after consumption of 50 mg iodine/iodide.

Notes
1. Abraham GE, Flechas JD, Hakala JC. Measurement of urinary iodide levels by ion-selective electrode: improved sensitivity and specificity by chromatography on an ion-exchange resin. Original Internist. 2004;11:19-32.
2. Abraham GE. The concept of orthoiodosupplementation and its clinical implications. Original Internist. 2004;11:29-38.
3. Abraham GE, Brownstein D. Validation of the orthoiodosupplementation program: A Rebuttal of Dr. Gaby's Editorial on iodine. Original Internist. 2005;12:184-194.
4. Abraham GE. The safe and effective implementation of orthoiodosupplementation in medical practice. Original Internist. 2004;11:17-36.
5. Brownstein D. Iodine: Why You Need It, Why You Can't Live Without It. West Bloomfield, MI: Medical Alternative Press; 2004.
6. Flechas J. The Iodine/Iodide Loading Test. Available at http://www.vrp.com/test-kits/the-iodine-iodide-loading-test. Accessed September 26, 2012.
7. WHO, UNICEF, ICCIDD. Assessment of iodine deficiency disorders and monitoring their elimination; a guide for programme managers, third ed. Geneva: WHO publications; 2007.
8. de Benoist B, McLean E, Andersson M, Rogers L. Iodine deficiency in 2007: global progress since 2003. Food Nutr Bull. 2008;29:195-202.
9. Ohashi T, Yamaki M, Pandav CS, Karmarkar MG, Irie M. Simple microplate method for determination of urinary iodine. Clin Chem. 2000;46:529-536.
10. Bartels H, Böhmer M. [Micro-determination of creatinine]. Clin Chim Acta. 1971;32:81-85. German.
11. Smyth PP, Duntas LH. Iodine uptake and loss-can frequent strenuous exercise induce iodine deficiency? Horm Metab Res. 2005;37:555-558.
12. Underwood EJ. Trace Elements in Human and Animal Nutrition. New York: Academic Press;1977.
13. The Iodine/Iodide Loading Test. Optimox Corporation. Available at http://www.optimox.com/pics/Iodine/loadTest.htm. Accessed September 26, 2012.
14. Abraham GE, Handal RC, Hakala JC. Simplified procedure for the measurement of urine iodide levels by the ion-selective eleectrode assay in a clinical setting. Original Internist. 2006;13:125-135.
15. Rasmussen LB, Ovesen L, Christiansen E. Day-to-day and within-day variation in urinary iodine excretion. Eur J Clin Nutr. 1999;53:401-407.
16. Rasmussen LB, Ovesen L, Bülow I, Jørgensen T, Knudsen N, Laurberg P, Perrild H. Relations between various measures of iodine intake and thyroid volume, thyroid nodularity, and serum thyroglobulin. Am J Clin Nutr. 2002;76:1069-1076.
17. Rasmussen LB, Carlé A, Jørgensen T, Knudsen N, Laurberg P, Pedersen IB, Perrild H, Vejbjerg P, Ovesen L. Iodine intake before and after mandatory iodization in Denmark: results from the Danish Investigation of Iodine Intake and Thyroid Diseases (DanThyr) study. Br J Nutr. 2008;100:166-173.
Financial Disclosure
 This study was independently funded by ZRT Laboratory. Currently, ZRT laboratory offers an iodine spot test using dried urine. Theodore Zava has an equity interest in ZRT Laboratory, a company that could potentially benefit from the publication of this study. This study was independently funded by ZRT Laboratory. Currently, ZRT laboratory offers an iodine spot test using dried urine. Theodore Zava has an equity interest in ZRT Laboratory, a company that could potentially benefit from the publication of this study.
Theodore Zava received his bachelor's degree in biology from Oregon State University in 2009. He is a research associate at ZRT Laboratory in Beaverton, Oregon, where he developed a test to measure iodine and creatinine levels in dried urine. His current research focuses on iodine deficiency/excess, Japanese iodine intake, halide competition, thyroid disorders, elemental analysis, and iodine kinetics in the human body.
Theodore Zava
Research Associate, ZRT Laboratory
ttzava@zrtlab.com
|



