| The
Basics of an Epidemic
What do chronic pain, diabetes, heart disease, menstrual difficulties,
and sleep apnea have in common? As physician Mark Starr points out
in his extensively researched book, Hypothyroidism
Type 2: The Epidemic, there's an excellent chance that this
apparently disparate collection of disorders – among literally
dozens, if not hundreds – indicate abnormally low thyroid
function.
The thyroid is a butterfly-shaped endocrine gland located at the
throat that produces numerous related hormones: thyroxin (also known
as T4), liothyronine (also known as T3), T2, and T1. T4, the most
well known of all the thyroid hormones, heats the body and speeds
metabolism (of fats, proteins, and carbohydrates) and heart rate.
T3, the most active form of thyroid hormone, also heats the body
and speeds metabolism and heart rate. At best, T4 is only about
one-quarter as potent as T3, and in any case, most is converted
into the more active T3 by the liver, kidneys, and other body cells.
T2 stimulates metabolism, while one animal study showed that T1
cools the body and slows the heart. Together, all four of these
related hormones probably act synergistically in ways that are not
yet fully understood.
Thyroid underactivity, commonly called hypothyroidism, was first
reported in London in 1875. According to many reliable sources,
including doctors Broda Barnes, David Derry, Jacques Hertoghe, and
James Howenstine, at least one-third to one-half of the US population
suffers from slight to severe hypothyroidism.

Before and after dessicated thyroid therapy
Source: Hertoghie, Eugene. The
Practitioner. Jan. 1915, Vol XCIV, No.
1.
Reprinted with permission.
In his book, Starr explains the differences between Types 1 and
2:
• With Type 1 Hypothyroidism, the thyroid does not produce
sufficient amounts of hormone to maintain "normal" blood
levels of hormones, which in turn will maintain normal blood levels
of thyroid-stimulating hormone (TSH) produced by the pituitary.
(I will say more about TSH a little later.)
• With Type 2 Hypothyroidism, the thyroid gland produces "normal"
amounts of hormone, but the cells are unable to utilize the hormone
properly. Some experts call this thyroid hormone resistance (which
may be regarded as similar to insulin resistance).
Laboratory tests showing inadequate bloodstream levels of thyroid
hormone make it easy to diagnose Type 1 hypothyroidism. However,
lab tests fail to detect Type 2 hypothyroidism, because despite
adequate bloodstream hormone levels, the cells are unable to accept
and utilize that hormone (for a variety of reasons, which I'll address
in a moment). Since the main problem lies with the cells that are
actually utilizing the hormone, a different approach needs to be
taken when testing for – and to a certain extent, when treating
– Type 2 hypothyroidism.
Since many more people suffer from Type 2 than Type 1 hypothyroidism,
and because Type 2 is widely misunderstood and misdiagnosed, this
article will focus on Type 2: its manifestations, the best way to
diagnose it (it's not with lab tests), and its treatment. For this
article, I have drawn heavily from Mark Starr's book, Hypothyroidism
Type 2: The Epidemic.
Dr. Starr became interested in the subject for both personal and
professional reasons. More than a dozen years ago, he embarked on
a quest to heal his own chronic pain, fatigue, and allergies after
receiving no relief from the majority of physicians with whom he
consulted. Professionally, while treating thousands of people who
suffered chronic pain alongside a wide range of disorders, he discovered
a pattern. The underlying cause or contributing factor to their
pain was low thyroid function. Dr. Starr's book is the result of
over a decade's worth of intensive research and writing about the
history, problems, politics, personnel, literature, case studies,
and treatment related to hypothyroidism. I had the opportunity to
visit Starr's new clinic, which is near my home, so at the end of
this article, I will also give a brief description of his practice.
Endless Disease Conditions
Most people (correctly) regard the thyroid as responsible for proper
metabolism. However, this gland plays a major role in hundreds of
bodily functions. Here is just a sample of the many symptoms and
conditions that can be caused, indirectly or directly, by an under-functioning
thyroid gland:
• Appetite disruption (heightened or diminished)
• Autoimmune conditions, including allergies, lupus, and rheumatoid
arthritis
• Blood sugar disorders, such as diabetes, hypoglycemia, or
a combination of the two
• Cancers, all kinds
• Cardiovascular abnormalities, including high cholesterol,
poor circulation, heart palpitations, hypertension (high blood pressure),
and hypotension (low blood pressure)
• Dental problems, including chronic gum infections, receding
gums, and TMJ or Temporomandibular Joint dysfunction (clenching
of the teeth, leading to chronic inflammation and pain in the temporomandibular
joint)
• Fatigue and lethargy
• Gastrointestinal disorders, including irritable bowel syndrome,
and impaired digestion leading to constipation and nutritional disorders
• Heart conditions, including coronary artery disease from
accelerated atherosclerosis (hardening of the arteries), arrhythmia
(irregular heartbeat), abnormal blood pressure (either too high
or too low), diminished cardiac output, weakness of the heart muscle,
and congestive heart failure
• Hoarseness of voice, difficulty in swallowing, swollen enlarged
tongue, and sleep apnea
• Immune response malfunction, leading to increased infections
(including Candida albicans) in all parts of the body
• Mental and emotional problems, including difficulty in cognition,
and anxiety, depression, memory loss, manic depression, psychosis,
and schizophrenia
• Metabolism malfunctions, leading to weight gain (usually)
or weight loss (occasionally)
• Muscular disturbances, including ataxia (lack of coordination),
carpal tunnel syndrome, fibromyalgia, and weakness
• Neurological impairment, including but not limited to ear
conditions (deafness, tinnitus, and vertigo), headaches and migraines,
Multiple Sclerosis, and paresthesia (numbness and "pins and
needles" in nerves)
• Pain in joints and muscles, including arthritis and fibromyalgia
• Perspiration reduction
• Reproductive disorders, including birth defects, cysts in
breasts and ovaries, endometriosis, infertility, and menstrual disturbances
• Respiratory conditions, including asthma, emphysema, pneumonia,
and chronic sinus infections
• Skin disorders, including acne, alopecia (hair loss), boils,
dryness, eczema, hives, and psoriasis
• Sleepiness and sleep apnea.
• Slowed movement and speech
• Structural weaknesses/deformities and impaired ability to
repair damaged tissues, manifesting in brittle nails, brittle or
scant hair (including baldness), degenerating bones (osteoporosis),
malformed bones (scoliosis), and thinning and loss of eyebrows,
notably the outer third
• Temperature regulation malfunction: intolerance to heat,
and excessive coldness, particularly in extremities.
• Urinary tract problems, such as urinary infections and especially
kidney failure from shrunken, scarred kidneys
Why So Many Conditions?
How is it possible that the malfunction of one tiny gland can influence
so many other functions that do not seem related to each other?
Consider the most obvious effect of an underactive thyroid: reduced
cell metabolism of proteins, fats, and carbohydrates. This not only
means inefficient transport of nutrients into the cell membrane,
but also inefficient transport of wastes out. As holistic practitioners
well know, inadequate nourishment and the buildup of toxins (regardless
of the cause) can exacerbate or outright cause virtually all conditions
that we call "disease." The more toxins engorge the cells,
the more one becomes susceptible to infections and degenerative
conditions. As it turns out, the mitochondria – microscopic
energy-burning units of the cell responsible for about 90% of the
energy production that our cells, tissues, and organs require for
metabolism – are intimately affected by thyroid dysfunction.
Starr writes:
Thyroid hormones are responsible for our
metabolism. When thyroid hormones are given to animals, trillions
of mitochondria increase in size and number. The total membrane
surface of the mitochondria increases almost directly in proportion
to the increased metabolic rate of the whole animal. My medical
school textbook, The Textbook of Medical
Physiology, states: "It seems almost to be an obvious
deduction that the principal function of thyroxin [thyroid hormone]
might be simply to increase the number and activity of mitochondria."
The beneficial symbiotic relationship between
mitochondria and thyroid hormone works both ways. Adequate levels
of thyroid hormone not only increase mitochondria number and function,
but as Starr points out, "mitochondrial mutations appear to
be largely responsible for the metabolic defects at the cellular
level, which result in a hypothyroid-like condition…. Defects
in mitochondria, as well as synthetic toxins, impair thyroid hormone
metabolism at the cellular level." Not surprisingly, symptoms
of mitochondrial disease are the same as symptoms of hypothyroidism.

Before and after desiccated thyroid therapy
Source: Lisser, H. and Escamilla, R.F. Atlas
of Clinical Endrocrinology: Including Text of Diagnosis and Treatment.
C.V. Mosby Company, 1957. Reprinted with permission.
There are scores of environmental toxins that interfere with every
aspect of thyroid metabolism and cause the mitochondria to malfunction.
These include petroleum and petroleum byproducts; pesticides, herbicides
and fungicides; heavy metals, among them mercury, arsenic, lead,
aluminum, barium, and cadmium; organic solvents, including benzene,
toluene, trichloroethylene, and dichloromethane; and numerous other
synthetic chemicals. Fat-soluble toxins lodge in the fat cells that
lie beneath the skin and surround internal organs. Women, whose
bodies contain more fat than men's, hold proportionately more toxins
in their systems and thus, one might assume, suffer from hypothyroidism
in much greater numbers than do men. Statistics show this to be
true.
Faulty thyroid receptors on the cell membranes as well as mitochondrial
mutations can cause a hypothyroid condition. "Defective thyroid
receptors," Starr writes, "may prevent a sufficient supply
of hormones that are circulating in our blood from reaching the
mitochondria and other crucial sites such as the nucleus of the
cell. The nucleus is where the thyroid hormones activate genes and
stimulate protein synthesis, among a host of other tasks" [emphasis
added]. This explains why so many people with underactive thyroids
have brittle nails and hair, and even bone defects. If the body
cannot utilize amino acids to create new, properly formed tissue,
the cells will be imperfect and cause structural abnormalities.
Myxedema, which is the retention of mucin, can also occur when the
tissues do not properly process and utilize thyroid hormone. (Myx
is the Greek word for "mucin," and edema means "swelling.")
Mucin is a compound comprised of sugars bound to a protein and in
modest amounts is a constituent of connective tissue. (Connective
tissue lines blood vessels, comprises nerve sheaths, is part of
the fascial envelope surrounding muscles, and is in organs and glands,
in the gastrointestinal and urinary tracts, and in the mucous membrane
lining of the respiratory tract, including the sinuses.) By nature,
jelly-like mucin absorbs water. When present in normal amounts,
mucin is not a problem. But in excess, the hydrophilic (water-loving)
mucin can cause serious problems wherever it accumulates in the
connective tissue. Over half of the hypothyroid population (55%-60%)
has abnormally high amounts of mucin, which accumulate more with
age. In fact, the medical term for "hypothyroidism" used
to be myxedema.
You can see how an underactive thyroid can be responsible for so
many debilitating and apparently disparate health problems. Just
a small sample includes heart disease, digestive disorders, liver
malfunction, lupus, muscular pain, neurological impairment, sinusitis,
and sleep apnea (caused by a swelling of the trachea and larynx).
Also worth noting are Temporomandibular Joint (TMJ) problems. These
often accompany hypothyroidism due to slow contraction and relaxation
of the muscles. Muscle spasms are common in hypothyroidism, as are
arthritic changes and joint effusions (an abnormal buildup of joint
fluid).
Inadequate thyroid hormone at the cellular level also negatively
impacts other glands. "Without the crucial influence of thyroid
hormones," Starr emphasizes, "proper maturation and function
of the other hormone glands is not possible." To compensate
for the weakness and low metabolism caused by inadequate thyroid
hormone, other parts of the body overwork, including the adrenals
and the sympathetic nervous system. This may cause the subject to
temporarily experience a rapid heartbeat and/or feel hyperactive,
jittery, and restless – until exhaustion sets in from the
unnatural attempts to compensate for low thyroid hormone levels.
More often, though, the majority of sufferers simply feel fatigued
and weak most of the time.
As you review the previous list of health conditions directly caused
or heavily influenced by hypothyroidism, keep in mind the phrases
poor utilization of thyroid hormone by the tissues, excess mucin,
and inadequate function of other glands. Just these three descriptions
can explain almost all of those symptom pictures.
Flawed Lab Tests
The biggest error in hypothyroid diagnosis is the medical profession's
excessive reliance on laboratory tests only, to the exclusion of
the subjects' symptoms. When hypothyroidism was first detected in
the 1800s, physicians listened to the people who actually had the
disorder and based their treatments on what they observed and on
what their patients told them. There are many physical signs of
hypothyroidism, among them puffy face and lips, hair loss, dry puffy
skin, abnormally slow movements and speech, hoarse voice, and intolerance
to cold. (Not only does the person subjectively feel chilly, but
the hands and feet feel cold to another person's touch.) Mark Starr
writes that in the early twentieth century,
…the ultimate test of whether or not
a patient was hypothyroid was the patient's response to a trial
of thyroid hormones. Confirmation depended upon improvement or
resolution of their symptoms. . . . [But] the list of thyroid
blood tests grew until there were scores of available tests. Unfortunately,
they failed to improve the ability to detect Type 2 hypothyroidism.
Today, the overwhelming majority of doctors are taught to check
only the patients' blood tests if they suspect hypothyroidism.
If the tests are normal, the search begins for other possible
causes of their problems. The vast majority of patients with hypothyroidism
have normal thyroid blood tests, because the tests do not detect
Type 2 hypothyroidism. Countless new syndromes, both mental and
physical, have been adopted in [futile] attempts to explain the
myriad symptoms related to hypothyroidism [emphasis added].
How ironic – though one must admit,
not surprising! – that with the mechanization of medicine,
along with its reductionist laboratory tests and synthesized pharmaceuticals,
the person's own experiences and symptoms became secondary to the
practitioner's theories. In the words of Starr, medical professionals
have become "blinded by their devotion to the laboratory tests."
Drawing on the groundbreaking (and commonsense) work of pioneer
physicians – including Broda Barnes, Eugene Cohen, Jacques
Hertoghe, Hermann Zondek, Hans Kraus, and Lawrence Sonkin (the latter
two with whom he studied) – Starr analyzes in depth some common
misconceptions about thyroid testing. The most commonly used blood
test, which is based on the theory of the TSH-thyroid hormone feedback
loop, contains a simple but major flaw. Since somany doctors rely
on this test to make an accurate diagnosis, it's worth addressing.
The most common blood test for hypothyroidism depends on the following
assumptions. The body tissues transmit their need for thyroid hormones
to the hypothalamus in the brain, which sends a signal to the pituitary
gland. In turn, the pituitary secretes thyroid stimulating hormone
(TSH), which signals the thyroid gland to secrete more hormones.
These hormones are then carried by the bloodstream to the tissues.
The action of the thyroid hormones on the tissues reduces the tissue
signals to the brain for more thyroid hormones, and the pituitary
stops secreting TSH.
The problem with this scenario is that most of the time, the mitochondria
in toxic and defective cells are unable to convey to the brain their
need for thyroid hormone, even if it's urgently required. In fact,
according to numerous studies, people whose mitochondria tested
abnormal nonetheless had normal thyroid hormone levels in their
blood. Modern thyroid blood tests, Starr reminds us, do not detect
Type 2 hypothyroidism "because thyroid hormone levels [in the
bloodstream] may be normal, but they are not high enough to stimulate
the . . . defective mitochondria into normal activity" [emphasis
added]. Nor are the blood thyroid hormone levels high enough to
induce the resistant receptor sites on the cells to start accepting
hormone. Any part of the cell can be involved in the failure to
process and utilize thyroid hormone. "There is no scientific
evidence," Starr bluntly states, after providing a detailed
review of the literature, "to support the doctors' claim that
the TSH test detects hypothyroidism in the vast majority of patients.
The validity of the TSH [tests] has been [solely] established by
word of mouth and [only] purportedly by the [flawed] studies I have
presented." Unfortunately, few medical personnel appear to
have read the literature upon which the presumed validity of the
TSH test was based – or have read it with a careful enough
analytic eye.

Before and after dessicated thyroid therapy
Source: Hertoghie, Eugene. The
Practitioner. Jan. 1915, Vol XCIV, No.
1.
Reprinted with permission.
 
Before and after dessicated thyroid
therapy
Source:Allbut, T.C. A System
of Medicine, London, Macmillan and Company,
1901. Reprinted with permission.
(Note: Photo on the left has been cropped.)
The Need to Observe
Clinical Symptoms
I have already mentioned the clinical observation of numerous signs,
such as puffy face and lips, thinning or lack of hair, the missing
third of the outside of the eyebrows, swollen skin, lack of alertness,
slowed speech, hoarseness, and cold extremities. And, of course,
there's the common weight gain and tendency toward chronic infections.
There is also another very simple hypothyroid indicator that was
developed by Broda Barnes, MD, PhD (he died in 1988). Barnes told
his clients to take their armpit temperature before rising every
day, usually over a period of weeks. If the temperature averaged
lower than 97.8º F, the person was considered hypothyroid.
Starr points out that the basal temperature test for hypothyroidism
is "not infallible" – for example, someone might
be hypothyroid but have a near-normal basal temperature, suggesting
that the higher-than-expected temperature readings may be due to
chronic inflammation in the lungs or elsewhere. Nevertheless, Barnes's
temperature test is still an effective and accurate diagnostic tool
in most instances.
Again, I refer the reader back to the extensive list at the beginning
of this article. By now, it should be clear that hypothyroidism
is fairly easy to detect, once you know what to look for. One more
thing: a prominent research study in the Journal
of Clinical Endocrinology found that some people with severe
biochemical hypothyroidism exhibited only mild clinical signs, whereas
others with minor biochemical changes exhibited severe clinical
signs.
These are the last "before" and
"after" pictures concerning hypothyroidism treatment that
Dr. Starr has seen in any endocrinology textbook. With all of the
subjects, the only thyroid hormone treatment
Top left: Woman
with abdominal fluid (ascites) before dessicated thyroid therapy.
Top right: The
same woman, no longer with ascites, after three months of
desiccated thyroid hormone therapy.
Middle left: Person
wioth enlarged heart before desiccated thyroid therapy.
Middle right: The
same person with a successful resolution of congestive heart
failure - a normalized heart - after three months of desiccated
thyroid hormone therapy.
Bottom left: Person
with enlarged and inflamed colon before desiccated thyroid
therapy.
Bottom right: The
same person, now with a normal colon, after three months of
desiccated thyroid hormone therapy. |
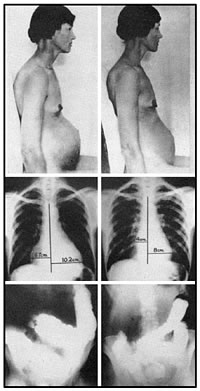 |
Source: Lisser, H., and Escamilla, R.F..
Atlas of Clinical Endocrinology:
Including Text of Diagnosis and Treatment.
C.V. Mosby Company, 1957. Reprinted with permission.
Treatment for Type 2 Hypothyroidism
1. Replacement Hormone
Whether the person's thyroid gland is not producing enough hormone
or the cells are unable (for whatever reason) to process what the
gland is producing, the treatment is the same: replacement hormone.
From the perspective of conventional medical training, flooding
the system with thyroid hormone, in amounts greater than what laboratory
blood tests might indicate are useful or prudent, may seem questionable.
But consider the highly dysfunctional state of the mitochondria
and/or cell receptors. If you saturate the tissues with enough hormone,
for a long enough period, even malfunctioning mitochondria and stubborn
receptor sites will start processing and utilizing the hormone.
Once the body begins to function correctly, it has the potential
to self-correct. Then, conceivably, the hormone dosage can be reduced.
This points to the need for careful monitoring of people with Type
2 hypothyroidism. It's easy to assess a body that is starting to
heal, Starr maintains. "The increased basal temperature that
results from administering desiccated thyroid is a direct result
of enhanced mitochondrial activity."
What type of pharmaceuticals work best? Up until the 1960s, people
suffering from hypothyroidism were given desiccated thyroid derived
from pigs. This means the entire dried gland and its contents –
all four forms of thyroid hormone, RNA, DNA, and other co-factors.
But by the 1970s, isolated thyroxin (T4) was introduced as the "gold
standard" of thyroid medications. By definition, thyroxin is
only a portion of the thyroid hormone complex. Since it does not
contain the synergistic effects of the entire glandular material,
not surprisingly, it proved less effective clinically than the desiccated
thyroid.
One such study on the superiority of desiccated thyroid over thyroxin
was conducted in Belgium and was published in 2001 by endocrinologist
Jacques Hertoghe and his colleagues in the Journal
of Nutritional and Environmental Medicine. Subjects showed
marked improvement when they began taking desiccated thyroid instead
of only T4. The hallmark symptoms of low thyroid – constipation,
headache, joint and muscle pain, muscle cramps, depression, cold
intolerance, and fatigue – were reduced by 70% after they
switched from T4 to desiccated thyroid. "Symptoms of the patients
already taking T4," notes Starr, reviewing the study, "did
not differ from those of the group of untreated patients" [emphasis
added].
Occasionally, Dr. Starr has found, some people require compounded
T3 or T4 only or combinations of the two, because they are either
allergic to, or unable to tolerate, desiccated thyroid. Or, they
don't want to take the desiccated pork product for religious reasons.
Whatever replacement hormone product is used, it's crucial that
the client be monitored on a regular basis. This includes self-monitoring.
The doctor must be willing to work closely with the client as well.
And the client must be willing and able to detect physiological
changes that indicate too little or too much hormone and regularly
report to the doctor.
Significantly, as one's metabolism becomes more efficient, perspiration
will increase, allowing for the elimination of more toxins. As more
toxins are eliminated, the better the cells – including the
mitochondria and hormone receptor sites – will function. This
suggests that mitochondrial defects can be corrected, given enough
time, patience, and dedication. (See below.)
2. Detoxification
Some of the most significant stressors of mitochondria are heavy
metals. Mercury is particularly insidious, as it's everywhere in
our environment and affects the system in devastating ways. It can
also be difficult to eliminate. Intravenous chelation therapy has
proven effective, but is expensive and time-consuming. Less expensive
but effective alternatives include the oral ingestion of broken
cell wall chlorella, liquid zeolite, alpha lipoic acid, and certain
amino acids in the correct proportions, often in combin ation with
each other.
The fact that a good portion of the T4 to T3 conversion takes place
in the liver also points to the need for a good detox liver protocol,
as this organ is primary in converting systemic and environmental
poisons into less noxious, more easily excretable substances. An
overall excellent – and easy – means of detoxifying
is sweating. Sweating reduces the waste removal burden on the kidneys,
liver, and eliminative organs. Numerous studies have shown vastly
decreased levels of mercury and other toxins after even only a few
weeks of regular sauna therapy. In fact, subjects have been known
to blacken their towels with the metals excreted through the skin
during sweating. My book, The Holistic
Handbook of Sauna Therapy, discusses sauna protocols in depth:
the mechanism of sweating; the three types of heat, including details
on far infrared; what types of heating elements and sauna building
materials are best for people with particular sensitivities and
needs; how to take a sauna and avoid heatstroke; which medical conditions
can be relieved by sweating; when one should not use the sauna at
all; and when one may use the sauna with medical supervision; pregnant
women and children in the sauna; and specific detox protocols.
Be aware that sauna therapy can achieve opposite effects with regard
to medication. On the one hand, some medication may be sweated out
of the system. On the other hand, the elimination of toxins increases
the metabolic efficiency of the cells, which means that in many
cases a drug is more efficiently absorbed into the cell –
and therefore will be needed in reduced amounts. Whatever detox
protocol you use, it needs to be consistent. Sometimes it can take
longer than desired to eliminate toxins from deep inside the tissues.
3. Nutritional Support
Iodine is essential for proper thyroid function. Potassium iodide
is absorbed directly by the thyroid gland, whereas iodine tends
to be more heavily concentrated in the breasts, reproductive organs,
and respiratory tract (including the sinuses). Both forms of iodine
are necessary for optimal functioning. Some types of seaweed added
to the diet, such as dulse, provide large quantities of iodine.
To assist in the conversion of T4 to T3, supplementation with selenium,
zinc, and vitamins E and B6 are usually indicated. Manganese, known
to protect the thyroid and liver, is sometimes called the "anti-pear
nutrient," so named because it helps eliminate the faulty weight
distribution pattern common with hypothyroid people. Thyroid hormone
increases the enzyme levels in the body. Since vitamins are essential
constituents of both enzymes and co-enzymes, increased thyroid hormone
levels require a higher intake of vitamins.
4. Glandular Support
Adrenal and thyroid function are intricately related. Sometimes,
hypothyroid subjects are unable to tolerate even sub-therapeutic
amounts of thyroid hormone due to adrenal fatigue. (In their attempt
to raise the energy of the body and compensate for the under-activity
of the thyroid gland, the adrenals have overworked and are now exhausted.)
Therefore, support for the adrenals, other glands, and even the
hypothalamus may be indicated during or even before beginning thyroid
hormone therapy.
Dr. Mark Starr's Clinic
In early 2008, Dr. Mark Starr left his established and thriving
pain clinic in Atlanta, Georgia, to relocate to Phoenix, Arizona.
In his spacious, comfortable, and conveniently located Paradise
Valley office, Starr continues to practice his specialty: the elimination
of pain and the treatment of hypothyroidism, usually with desiccated
thyroid hormone. (Some people are allergic to pork, are vegans,
or have religious objections to pork, so they take the compounded
pharmaceuticals.) Starr also specializes in sports injuries, using
FDA-approved and FDA-cleared electromedical devices that include
a state-of-the-art laser and the Tennant Biomodulator®.
As an author in the holistic health field who specializes in electromedicine,
I was very impressed with the range of therapies available in Dr.
Starr's clinic. I was also impressed with Starr's knowledge, obvious
passion, caring, and dedication to helping people regain their health.
Having dealt with his own hypothyroid issues and been obliged to
dig for answers that at the time were not readily available, Dr.
Starr makes an excellent advocate for those seeking competent medical
treatment.
Summary
Dr. Mark Starr's extensively researched book, Hypothyroidism
Type 2: The Epidemic, is essential reading for both professionals
and laypersons. The book cites long-term studies, involving thousands
of subjects, showing that hypothyroidism is rampant. Starr's book
also explains how Type 2 hypothyroidism develops and describes the
best treatments for it. Physicians in all specialties who want to
augment the efficacy of their care should read Dr. Starr's book.
The many photographs in the book of hypothyroid people, before and
after treatment with thyroid hormone, reinforce the differences
between hypothyroidism and normalcy in an unmistakable and striking
way. Anyone who looks at these "before" photographs is
bound to recognize someone they know – someone who could have
been helped to overcome a debilitating condition, if only they or
their doctors knew about it.
Unfortunately, hypothyroidism is often the last possibility considered
for those who are unwell. Since thyroid hormones are intricately
related to virtually every bodily function, hypothyroidism can cause
or exacerbate an almost unlimited number of conditions that initially
might not seem related to each other. This points to the importance
of applying an integrative approach to how the body functions, instead
of perceiving various conditions as discrete "diseases."
Laboratory tests for hypothyroidism miss the vast majority of sufferers.
The most commonly performed, "gold standard" tests do
not reveal what is occurring at the cellular level. If the cells
are unable to utilize and process thyroid hormone, even with normal
bloodstream thyroid hormone levels, the person has hypothyroidism
– in this case, Type 2, which is pervasive in a large percentage
of the population and unrecognized by mainstream medicine.
The client's history and clinical exam are the best diagnostic tools
for hypothyroidism: in fact, they are the basis of good medicine.
If the person's clinical picture improves when he or she takes thyroid
hormone, then he or she is hypothyroid! This simple concept can
be difficult for some professionals to grasp, especially if they
insist on ignoring their clients' symptoms at the expense of erroneous
theories. As Dr. Thomas Boc remarks: "There are countless thousands
of people who are in failing health because their doctors are not
listening to what the patient is trying to tell them about their
illnesses. They [the doctors] have been trained to rely on blood
tests more than on the history and examination of the patient."
Desiccated thyroid is more effective than T4 (levothyroxin) for
treating hypothyroidism. Prominent studies prove that heavy metals,
especially mercury, interfere with thyroid hormone uptake and utilization.
Therefore, detoxification protocols such as chelation and sauna
therapy are indispensable. So is proper nutrition, including supplementation
with iodine and other minerals like selenium, without which thyroid
hormone cannot be utilized and converted into a form useable by
the tissues. As the body eliminates toxins and nutrient absorption
is improved, the thyroid hormone dose may need to be decreased.
Thus, care must be taken to monitor the client's responses.
It's critical that health practitioners learn how to diagnose and
treat Type 2 hypothyroidism. The ability to work with this condition
indicates a caring, open-minded, and competent professional who
is free from rigid and antiquated notions that do not reflect the
lives, suffering, or medical conditions of real people. Clients
fortunate enough to obtain proper treatment for hypothyroidism enjoy
a vastly improved quality of life – physically, mentally,
emotionally, and spiritually.

Proper Thyroid Supplementation
Prevents Heart Attacks
[In 1948], the National Heart
Institute began the Framingham Study, officially named "The
Heart Disease Epidemiology Study." The objective: to determine
why heart attacks were rapidly reaching epidemic proportions.
Over 5,000 adult residents of Framingham, Massachusetts volunteered
to participate in the long-term medical study. The group underwent
thorough physical exams. All were free of heart disease initially.
Participants were examined at two-year intervals. People who later
suffered heart attacks helped determine the so-called “risk
factors” that became associated with the illness. Risk factors
included high blood pressure, elevated cholesterol, increasing
age, and having a family history of heart attacks. Men were found
to be at higher risk of heart attacks than women.
In 1950…Dr. [Broda] Barnes began a long-term study to determine
if proper treatment of hypothyroidism would prevent heart attacks….
Dr. Barnes intended for his study to parallel the Framingham Study….
[His] research included 1,569 patients who received treatment
for their hypothyroidism. A minimum of two years of thyroid therapy
was required to be included in the study…. An individual
patient’s symptoms, response to the hormones, and basal
temperatures determined their dosage of thyroid hormones….
The Framingham Study would have predicted that 72 of Dr. Barnes’s
patients should have suffered heart attacks. Only four occurred….
Dr. Barnes purposely did not attempt to control cholesterol, smoking,
exercise, or other variables among his study group. He wanted
the only variable between his patients and those from the Framingham
Study to be the use of thyroid hormones….
Over 90% of predicted heart attacks from the Framingham Study
were prevented…. Dr. Barnes predicted that our massive effort
to control heart attacks would fail, unless we recognized and
properly treated hypothyroidism.
– Mark Starr, MD(H)
Hypothyroidism Type 2: The Epidemic
(2007), 34-35
To contact Dr. Starr:
Mark Starr, MD(H)
21st Century Pain & Sports Medicine
10565 North Tatum Boulevard, B115
Paradise Valley, Arizona 85253
480-607-6503
www.21centurymed.com
Notes:
1. Starr M. Hypothyroidism Type E: The
Epidemic. Irvine, CA: New Voice Publications; 2005, 2007:
55.
2. Starr 59, 69.
3. Starr 61.
4. Starr 1.
5. Starr 63–64.
6. Starr 71.
7. Starr 59.
8. Starr 70.
9. Starr 137.
10. Starr 59.
11. Starr 175.
12. Starr xvi
© 2008 by Nenah Sylver, PhD
Nenah Sylver, PhD
P.O. Box 74324
Phoenix, Arizona 85087-4324
nenah@nenahsylver.com
www.nenahsylver.com
Book Orders Only:
845-687-4184
www.bibliotique.us/si/sauna.html
(The Holistic Handbook of Sauna
Therapy) or
www.bibliotique.us/si/rife.html
(The Rife Handbook of Frequency
Therapy)
|



